“Tendinitis,” or the more comprehensive/accurate term “tendinopathy” is of the most common overuse injuries that we see in physical therapy. Whether “jumper’s knee” (patellar tendinopathy”), Achilles’ tendon pain, or plantar fasciitis (fasciopathy or heel pain); these injuries are incredibly common and often very painful and debilitating.
In working with many patients with these conditions, I would like to share some clinical tips in assessing and treating that I have gleaned from my experience and from my reading.
*Note: For a more in depth discussion of pathophysiology, diagnosis and treatment rationale for lower extremity tendinopathy, please reference these posts:
Tips for Treating Lower Extremity Tendinopathies: Part 1: ASSESSMENT
Tips for Treating Lower Extremity Tendinopathies: Part 2: EXERCISE PRESCRIPTION
Tips for Treating Lower Extremity Tendinopathies: Part 3: INDIVIDUALIZING TREATMENT (CASE EXAMPLES)
Gluteal Tendinopathy/Greater Trochanteric Pain Syndrome
My Big 3 Tendinopathy Treatment Tips:
- Test for Load Tolerance
- Progress Load Over Time
- Load with an End Goal in Mind
1- TEST FOR LOAD TOLERANCE
Testing for load tolerance can inform diagnosis and guide treatment for tendinopathies, especially if using “pain provocation” tests as part of a physical therapy evaluation and using a “pain monitoring model” as a guideline for exercise prescription (i.e., keep pain < 4/10 with exercises and activity).
The word tendon comes from the Latin Tendere (“To Stretch”), reminding us that tendons are designed to take tensile loads. However, tendons are sensitive to “overloading” if not given enough recovery between loads and this could be one explanation for developing tendon pain (i.e., “tendinitis” or “tendinopathy”).
Some of the same loading tests that a physical therapist may use to diagnose a tendinopathy issue can be used to guide the best therapeutic loads for strengthening the tendon (or around the tendon). See below for a “Cheat Sheet” with common load tests for diagnosing and assessing load tolerance for lower body tendinopathy:
LOWER LIMB TENDINOPATHY LOAD TESTS & SPECIAL TESTS
Just like other tissues in our body (think muscle and bone), tendons adapt to the loads placed on them and so prescribing an appropriate load is part of the key to successful rehabilitation.
The ideal load to ensure healthy tendons is somewhere between “under loading” and “overloading”
Load prescription in tendinopathy rehabilitation is best guided by a “pain monitoring model”, where the goal is to keep the person’s pain below a 3/10 with all exercises and activities (Silbernagel, 2007); I usually allow up to 4/10 pain for most patients.
2-PROGRESS LOAD OVER TIME
In rehabilitation for tendinopathy, the goal is to prescribe exercises and activities that will strengthen and increase capacity of the muscle-tendon unit while being careful not to cause overload or a “flareup” in symptoms. This means deliberately and intentionally progressing certain key loading variables over time (e.g., type of load, volume, weight/intensity, and speed).
Early on manipulating the type of load can be extremely helpful. For example, long hold isometrics may be better tolerated by a patient with highly irritable symptoms. As symptoms decrease, there can be progression to isotonic (concentric and/or eccentric) exercises (see figure below):
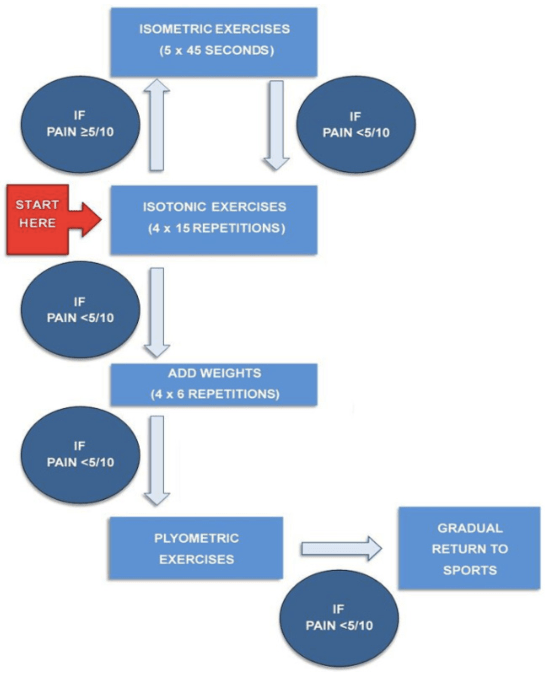
Besides type of loading, other important variables to consider are the volume, weight, and speed of loading. It is particularly important to build a strength base or tolerance to moderate to heavy loads before introducing high speed loads. Early on in treatment, most tendon pain will not respond favorably to quick loading or fast stretch-shortening cycles at the muscle-tendon unit (e.g., running, jumping, plyometrics). Effective progression of loads to treat tendinopathies generally follows the sequence below:

An appropriately high load must be undertaken in order to see improvements in tendon pain. So-called “heavy slow resistance training” paradigms have been shown to be just as effective as popular eccentric training programs for Achilles’ tendinopathy rehabilitation (Beyer, 2015). One study using this approach progressed the weight used for single leg calf raises over a 12-week training period. Weight used was gradually increase and repetitions were decreased (starting with 3×15 and progressing to 3×4-6).
From strength and conditioning research, it is apparent that working at a 15-repetition maximum will place the load for an exercise at approximately 65% of a 1 repetition maximum (1RM) lift, which is what is commonly thought of as the minimum percentage/weight to use to see muscle strength gains.
Newer research on loading programs for tendinopathy indicates that training at a “moderate” intensity (defined as > 55% of 1RM) may be sufficient to see improvements in function, pain, and tendon structure (Agergaard, 2021). In one study on patellar tendinopathy, there were no differences in improvements between a “heavy slow resistance training” group (trained using 90% 1RM load) versus a “moderate slow resistance training” group” (trained using 55% of 1RM) (Agergaard, 2021).
If prescribing exercise for tendinopathy and the individual can perform more than 15-20 repetitions, the weight is likely too light (< 55-65% 1RM). Using this repetition threshold is often useful in the clinic where testing for a true 1RM is often impractical, but one can also use a percentage chart to estimate a 1RM and prescribe weights accordingly.
See Below for 2 versions of a 1RM percentage chart:
Baechle & Roger 1RM PERCENTAGE CHART
The last point to consider is that tendinopathy load progression must be GRADUAL and rehabilitation for these conditions usually takes multiple months. Most tendinopathy treatment guidelines recommend A MINIMUM OF 12 WEEKS OF PROGRESSIVE LOADING before considering alternative treatment options (de Vos, 2021; Millar, 2021).
This could be partially because tendons may take 12 weeks to adapt to loading and remodel. One systematic review looking at prognosis for Achilles’ Tendinopathy concluded that there could be tangible improvements in symptoms and function by 4 weeks, but IMPROVEMENTS PEAKED AROUND 9-12 WEEKS after starting rehabilitation (Murphy, 2018).
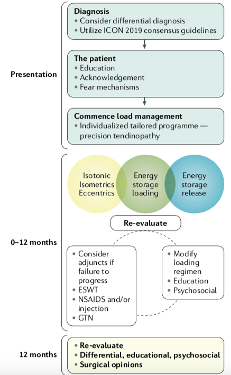
See Below for a recommended treatment progression for tendinopathy (up to 12 months of conservative treatment with re-evaluation!):
3-LOAD WITH AN END GOAL IN MIND
It may sound obvious, but keeping in mind the activities that an individual wants to return to can guide load prescription. The end goal of physical therapy is to return to sport, work, or any other recreational activity or daily activity the patient finds valuable (and that is realistic!).
These “end goals” (e.g., return to basketball, running, hard labor job, walking for exercise etc.) can then help to inform the intermediate goals and strength/load thresholds that must be achieved along the way.
I find having strength “thresholds” or goals in mind helps with progression of return to sport and even deciding when it is appropriate to progress from moderate/heavy resistance training to adding plyometrics or running/jumping. See below for a chart with some of my strength goals for different tendinopathies:
LOWER LIMB TENDINOPATHY STRENGTH GOALS
References:
Agergaard AS, Svensson RB, Malmgaard-Clausen NM, Couppé C, Hjortshoej MH, Doessing S, Kjaer M, Magnusson SP. Clinical Outcomes, Structure, and Function Improve With Both Heavy and Moderate Loads in the Treatment of Patellar Tendinopathy: A Randomized Clinical Trial. Am J Sports Med. 2021 Mar;49(4):982-993.
Beyer R, Kongsgaard M, Hougs Kjær B, Øhlenschlæger T, Kjær M, Magnusson SP. Heavy Slow Resistance Versus Eccentric Training as Treatment for Achilles Tendinopathy: A Randomized Controlled Trial. Am J Sports Med. 2015 Jul;43(7):1704-11.
de Vos RJ, van der Vlist AC, Zwerver J, Meuffels DE, Smithuis F, van Ingen R, van der Giesen F, Visser E, Balemans A, Pols M, Veen N, den Ouden M, Weir A. Dutch multidisciplinary guideline on Achilles tendinopathy. Br J Sports Med. 2021 Jun 29:bjsports-2020-103867.
Millar NL, Silbernagel KG, Thorborg K, Kirwan PD, Galatz LM, Abrams GD, Murrell GAC, McInnes IB, Rodeo SA. Tendinopathy. Nat Rev Dis Primers. 2021 Jan 7;7(1):1.
Morrissey D, Cotchett M, Said J’Bari A, Prior T, Griffiths IB, Rathleff MS, Gulle H, Vicenzino B, Barton CJ. Management of plantar heel pain: a best practice guide informed by a systematic review, expert clinical reasoning and patient values. Br J Sports Med. 2021.
Murphy M, Travers M, Gibson W, et al. The prognosis for mid-portion Achilles tendinopathy with rehabilitation: A systematic review and longitudinal meta-analysis. Journal of Science and Medicine in Sport. 2018;21:S83.
Silbernagel KG, Thomeé R, Eriksson BI, Karlsson J. Continued sports activity, using a pain-monitoring model, during rehabilitation in patients with Achilles tendinopathy: A randomized controlled study. The American Journal of Sports Medicine. 2007; 35(6):897-906.

4 Comments Add yours