
Groin injuries including adductor or hip flexor muscle strains are common in sports such as soccer, football, and hockey. These injures often occur following forceful cutting, sprinting, or kicking involved in these sports that places high stress on these muscle groups. The mechanism of injury, similar to hamstring strain injuries, often involves quick deceleration force or eccentric loading of the muscle.
Adductor muscle injuries can also include concurrent abdominal strain injuries due to the common attachment sites at the pubic bone and shared fascia from abdominal muscles (rectus abdominus) and adductor muscles (adductor longus) (Ellsworth, 2014). Multiple terms have been used interchangeably to describe this type of injury including “Athletic pubalgia”, “Sport’s hernia”, Gilmore’s groin. Though, it is important to note that this condition (i.e., “Sport’s hernia”) is not a true hernia (no organ protrusion through the abdominal wall), but instead a muscle, tendon, and/or fascial injury.
It has been reported that up to two thirds of groin injuries have some involvement of the adductor muscles. Adductor injury is the most common cause of groin pain in soccer players (Haroy, 2017) and in one sample of semi-professional male soccer players, 20% suffered a groin injury during the season (Haroy, 2019). Most commonly injured muscles in acute groin injuries are the rectus femoris, adductor longus, and iliopsoas and injury could include the muscle, musculotendinous junction, or the enthesis (tendon-bone attachment site) with presence of an avulsion fracture (Thorborg, 2018).
Can I Get Back to Playing Sports? And…How Long Will It Take?
Luckily, most acute adductor strain injuries have good prognosis for return to sport. Approximately 50% to 80% of athletes are able to return to sport after undergoing rehabilitation for adductor related groin pain. (Holmich, 1999; Serner, 2020; Weir, 2011). Even after surgical treatment for athletic pubalgia (often repairing damaged muscles, inguinal canal, etc.) return to prior function has been reported as high as 97% (Rabe, 2010).
Time to return to sport is variable and based on severity and chronicity of injury. If a strain is more acute and immediately treated, prognosis and recovery are faster. With chronic injuries (pain > 2-3 months) or more severe injuries involving avulsions or full tears, recovery may take longer.
In one sample of athletes with acute adductor strain injuries, those with a low to moderate severity of injury (graded with MRI) were able to return to full sports participation in approximately 2-3 weeks Serner, 2020).
The average time for return to sport if suffering from a chronic adductor/groin strain injury (pain > 2 months), return to sport timeframes have been reported as (median time for return to sport):
- 8.5 weeks (range 13-26 weeks) (Holmich, 1999)
- 13-17 weeks (Weir, 2011)
- 2-3 months (Serner, 2020)
Proposed Causes:
One proposed cause for adductor muscle strains is weakness of the adductor muscle group, which has been found in individuals with these injuries (Haroy, 2019; Moreno-Perez, 2019). In the case of “Athletic pubalgia,” or concurrent adductor and rectus abdominus injury, muscle imbalance may be present between stronger adductors and weaker abdominal muscles, causing excess forces around the attachments at the pubic tubercle on the pelvis (Abouelnaga, 2019; Rabe, 2010; Zuckerbraun, 2020). Those with chronic groin pain have also been found to have altered core muscle activation and specifically delayed onset of transversus abdominus muscle activation; though it is not certain whether this is causative or as a result of the painful condition (Cowan, 2004).
Differential Diagnosis of Groin Pain:
Diagnosing muscle strain injuries should include a comprehensive clinical examination, including screening for more sinister pathology. Presence of muscle strain related groin pain tends to be a ‘diagnosis of exclusion’ and other pathologies that should be considered are listed below.
Differential diagnosis of groin pain should include:
“Groin Pain Syndrome”*: defined as “Non hernia, Non hip groin pain” (Zuckerbraun, 2020)
- Has been called “Sport’s hernia”, “Athletic pubalgia”, “Gilmore groin”, “Sports man’s groin”, “inguinal disruption”, “core muscle injury” (can include injury to adductor or abdominal muscles, fascia and/or tendons)
Adductor Muscle Strain*: could include tendon injury and/or avulsion fracture (bone pulls away at the tendon attachment site) of one or multiple adductor muscles (adductor longus, adductor brevis, adductor magnus, pectineus, gracilis)
Hip Flexor Muscle Strain*: could include tendon injury and/or avulsion fracture (bone pulls away at the tendon attachment site) of one or multiple hip flexor muscles (rectus femoris, sartorius, tensor fascia latae (TFL), psoas, iliacus)
Osteitis Pubis: inflammation of the pubic symphysis (“non-infectious”, distinctly different than osteomyelitis). Patients often present with “waddling gait”, history of recent abdominal or groin surgery or trauma, and symptom reproduction with tests that load the pubic symphysis (+ “pubic spring test”, + FABER test, + lateral compression test, + adductor squeeze test) (Gomella, 2017)
“True” Groin Hernia: defined as “a protrusion of a portion of an organ or abdominal content through an abdominal opening in the groin area” Burcharth, 2014) and named for the opening where protrusion occurs: inguinal hernia or femoral hernia are most common (inguinal hernia is most common in males,
- A high majority of hernias are inguinal hernias (> 90% in one review, Burcharth, 2014)
Hip Joint or Lumbar Spine referred pain: These will be important to rule out and my specific testing or screening for these areas often includes: standing spine motions, squat to assess hip joint loading, quadrant testing for the lumbar spine and special tests at the hip such as scour test, quadrant tests, FADIR and FABER testing, and spine joint mobility assessment with central and unilateral anterior to posterior mobilizations (CPAs and UPAs)
Inguinal neuralgia: suspect nerve involvement if there is burning or shooting pain or paresthesia are present in the groin area. Nerves providing sensory innervation to this area that could be affected are ilioinguinal, iliohypogastric, or genitofemoral (Zuckerbraun, 2020)
Visceral or genitourinary systems referred pain: screening for these contributors to pain or symptoms will mostly be via subjective questioning and could include such factors as insidious onset of symptoms, urinary dysfunction, sexual dysfunction, abdominal pain reproduced around mealtimes, etc.
*Note: With clinical exam, pain or symptoms will be present with active contraction and passive stretch of an injured muscle or tendon, according to the Cyriax model of diagnosing contractile tissue injuries (Cyriax, 1982)
Groin Strains
The rest of this post will be focused on the diagnoses that fall under “Groin Pain Syndrome” or groin strains including adductor or hip flexor muscles with or without abdominal muscle involvement (e.g., “Athletic Pubalgia). This is also referred to as “adductor related groin pain”.
Common signs and symptoms of “muscle related groin pain” include: (Abouelnaga, 2019; Zuckerbraun, 2020)
- Symptoms located at the groin or anterolateral thigh
- Onset of symptoms with sprinting, cutting, or forceful kicking motion
- Pain with quick movements such as cutting, twisting, or sprinting
- Pain with getting in and out of a car
- Pain with lifting the legs up onto the bed or turning in bed
- Pain with sitting for long durations
- Pain with coughing/sneezing or bracing/Valsalva
- Pain with resisted hip adduction, adduction squeeze test (Moreno-Perez, 2019), sit-up or crunch motions
- Tenderness to palpation at the pubic tubercle and at any affected muscles/tendons (e.g., adductor, hip flexor, or abdominal muscles), could have tenderness at the inguinal ligament
- Negative testing at the lumbar spine and hip joint
Prevention: “Add” this exercise to your warmup!
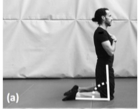
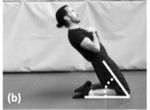
Research has shown that performing strength exercises for hip adductor muscle group, such as the “Copenhagen Adductor” exercise can reduce risk of groin injury in male soccer players
(Haroy, 2019). In one study, soccer players did this exercise (one of three variations) three times per week during their preseason (6-8weeks) and then continued to perform it once per week once in their competitive soccer season (28 weeks). Prevalence of groin injury was 41% lower in the group that did this exercise vs. a control group that did not!

(Figure above from Haroy, 2019)
Also, it has been shown that adding this one exercise to a common injury prevention program for soccer players (FIFA 11+), improved hip adduction eccentric strength over the course of 8 weeks (used 3 times a week within warmups) (Haroy, 2017). Even training with this exercise twice per week for 8 weeks (starting with 2 sets of 6 and progressing to 3 sets of 15) has been shown to significantly increase eccentric strength of the hip adductors (Ishoi, 2016).
Furthermore, preventing future strains (“secondary” injury prevention) is important after an initial groin related injury. In one study, undergoing criterion-based rehabilitation after an acute adductor strain injury reduced the risk of future adductor injury. This included the progression of exercise loads and speed as athletes meet functional milestones while keeping pain < 3/10 for all exercises and activities. (Serner, 2020).
Treatment for Athletes with Adductor Related Groin Injury:
First line treatment for groin pain (non-hernia and non-hip pathology) is usually conservative and can include rest, medication or pain reducing modalities, and physical therapy or exercise-based treatments. Exercise prescription is guided by symptoms, but goals include strengthening hip and abdominal muscles, improving flexibility of these muscles and the surrounding fascia and soft tissue structures, and optimizing core stability (Abouelnaga, 2019; Zuckerbraun, 2020). Ultimately, training and exercises progress to restoring the individual to functional movements and sports participation if applicable.
Research suggests that active treatments (progressive hip and core strengthening and stability exercises) added to “conventional treatment” (heat, massage, TENS, mobilizations) are superior to conventional treatment alone in improving pain and successful return to sport following sports hernia (Abouelnaga, 2019; Holmich, 1999). Athletes in the “active treatment group” returned to sport at a much higher percent and many reported no pain at follow up vs. “passive treatment” group) (Holmich, 1999).
If tendons are affected (from adductors or abdominal muscles), treatment strategies could include corticosteroid injections or PRP injections (Zuckerbraun, 2020). As mentioned above, usual care indicates conservative treatment, but if 6-8 weeks of this does not improve symptoms and function, surgery could be the next treatment option (Rabe, 2010). Surgical treatments may include reinforcement or repair of inguinal canal structures and/or muscle or tendon damage as necessary (with or without mesh reinforcement) or could include adductor tenotomy (Zuckerbraun, 2020).
Similar to a discussion of lower extremity tendinopathy loading progression*, exercise prescription often begins with isometric loading and progresses to isotonic (concentric and eccentric loading) as tolerated. Faster loading or movements (e.g., plyometrics or running/jumping) are introduced last and then sports specific movements can be integrated.
*Note: For more on lower extremity tendinopathy, please reference these posts:
Tips for Treating Lower Extremity Tendinopathies: Part 1: ASSESSMENT
Tips for Treating Lower Extremity Tendinopathies: Part 2: EXERCISE PRESCRIPTION
Tips for Treating Lower Extremity Tendinopathies: Part 3: INDIVIDUALIZING TREATMENT (CASE EXAMPLES)
Utilizing exercises from successful research protocols for rehabilitating adductor strain injuries (see: Abouelnaga, 2019; Haroy, 2019; Haroy, 2017; Holmich, 1999; Serner 2020; Serner, 2014; Weir, 2011; Zuckerbraun, 2020), along with my clinical experience in treating individuals following groin strain injuries, these have been some of the exercise progressions that I have utilized:
Weeks 1-4 following injury:
Goals: Initiate muscle contraction at tolerable levels, begin training for neuromuscular control of core muscles, emphasize isometrics and aerobic conditioning with walking, swimming (could be arms only ‘pulling’) or stationary bicycle as pain allows.
Example Exercises:
Core Control/Postural Awareness Exercises:
- Posterior Pelvic Tilts (hook lying progressing to seated)
- Transverse Abdominus Activation
- Sitting on Physioball
- Core Control, balance, proprioception- rows sitting on physioball, marches sitting on physioball, ½ kneeling and full kneeling anti-rotation presses (“Paloff Presses”)
Muscle Specific Exercises:
Isometric Holds:
5-10 sets of 30 second holds
(can use “effort based” % starting as low as 25% effort and progressing to 100% as tolerated)
- Adduction Isometrics:
- Ball squeeze at knees: Supine with knees bent to 90 degrees: squeezing a soccer ball between the knees
- Dose: 5-10 sets of 30 second holds (can use “effort based” % starting as low as 25% effort and progressing to 100% as tolerated)*
- Ball squeeze at feet: Supine with legs straight: squeezing a soccer ball between the feet
- *Dose: same as above
- Ball squeeze at knees: Supine with knees bent to 90 degrees: squeezing a soccer ball between the knees

Adductor Isometric 
Adductor Isometric
- Abdominal Isometrics:
- Partial Crunch Holds: Supine with knees bent to 90 degrees: slide hands midway up thighs and hold in this position
- *Dose: same as above
- Partial Oblique Crunch Holds: Supine with knees bent to 90 degrees: reach hand across to opposite thigh, slide hand midway up thigh and hold this position
- *Dose: same as above
- Partial Crunch Holds: Supine with knees bent to 90 degrees: slide hands midway up thighs and hold in this position

Partial Crunch Hold 
Oblique Crunch Hold
- Hip Flexor Isometrics:
- Knee March Supported: Supine with knees bent to 90 degrees: keeping feet flat on the ground, the patient will pull the knee up towards their chest but resist the motion by pushing down with their hand
- *Dose: same as above
- Knee March in “Tabletop Position”: Supine with hips bent to 90 degrees and knees bent to 90 degrees: keeping shins parallel with the ground, the patient will pull the knee up towards their chest but resist the motion by pushing down with their hand
- *Dose: same as above
- Knee March Supported: Supine with knees bent to 90 degrees: keeping feet flat on the ground, the patient will pull the knee up towards their chest but resist the motion by pushing down with their hand
Once isometrics are tolerated to at least 50% effort, isotonics should be introduced. I will use a similar “pain monitoring” model and recommend keeping pain < 4/10 during and immediately after exercises.
Weeks 2-6 following injury:
Goals: Progress isotonics (concentric and eccentric) for core and hip strengthening, add functional movement patterns emphasizing double leg squatting and deadlifting, adding lunge type movements if possible, conditioning with walking, swimming, biking, early return to run if tolerable
Higher repetitions, lighter weight (e.g., 3-5 sets of 10-15 repetitions)
Example Exercises:
- Partial sit-ups and oblique (rotational) sit-ups
- Side lying leg lifts of top and bottom leg (Hip abduction and adduction)
- Supine straight leg lifts (Hip flexion)
- Standing hip strengthening with band or cable weight resistance (flexion, abduction, adduction, extension)
- Double leg squats
- Sides steps with or without band resistance
- Modified planks
- Eccentric Control exercises:
- Eccentric Hip abduction with slide board or “carpet slider”
- Reverse Nordic hamstring exercise (If treating hip flexor strain)*
- Light dynamic warmup (< 75% speed)
- Light load/light intensity medicine ball chest pass or overhead throws
*Note: Reverse Nordic hamstring exercise increased fascicle length, muscle cross sectional area, muscle thickness, and pennation angle, in rectus femoris muscles after 8 weeks of training (progressing sets and repetitions from 2 sets of 6 up to 3 sets of 10-12 at end stage training; Note that changes reversed after 4 weeks of detraining) (see below, Alonso-Fernandez, 2019):

(Reverse Nordic Hamstring Exercise, Alonso-Fernandez, 2019)
Weeks 6-10 following injury:
Goals: Progress weight for double leg isotonics, add single leg movements like single leg squats and deadlifts, multidirectional lunges and higher speed movements such as plyometrics and return to running progressions, conditioning with walk/jog intervals, biking intervals, early multidirectional training and agility training
Higher repetitions, lighter weight (e.g., 3-5 sets of 10-15 repetitions)
Example Exercises:
- Copenhagen Hip Adduction exercise
- Plank variations, can add dynamic planks with leg or arm lifts or plank holds on unstable surfaces like a BOSU ball or gymnastics rings
- Longer lever core isometrics or isotonics with adduction holds (superman, hollow body, or tabletop positions)
- Chops and lifts (diagonal band pulls or weighted motions)
- Bird dogs
- Dead bugs or straight leg lowers
- Multidirectional lunges
- Split squats or single leg deadlifts
- Eccentric Control exercises: can progress repetitions/volume
- Dynamic warmup (progressing to > 75% speed)
- Cutting drills, agility drills, plyometrics
- Higher intensity medicine ball throws in rotational patterns

Table Top Hold orLower 
Long Lever Crunch or Toss 
Superman Hold 
Superman Hold with Add Squeeze
After 8-10 weeks progression of exercises and return to run may be variable and can be regulated based on pain response and competence with loading in movement patterns discussed above (squat, deadlift, walk/jog, and adductor and core specific exercises).
I hope this post has helped provide some context and tips for rehabilitation decisions following muscle related groin injuries.
Remember that this blog should not be taken as medical advice: please consult a licensed health care provider if you have experienced an injury for your individual medical needs.
References:
- Abouelnaga WA, Aboelnour NH. Effectiveness of Active Rehabilitation Program on Sports Hernia: Randomized Control Trial. Ann Rehabil Med. 2019 Jun;43(3):305-313.
- Alonso-Fernandez D, Fernandez-Rodriguez R, Abalo-Núñez R. Changes in rectus femoris architecture induced by the reverse nordic hamstring exercises. J Sports Med Phys Fitness. 2019;59(4).
- Burcharth J. The epidemiology and risk factors for recurrence after inguinal hernia surgery. Dan Med J. 2014 May;61(5):B4846.
- Cowan SM, Schache AG, Brukner P, et al. Delayed onset of transversus abdominus in long-standing groin pain. Medicine and Science in Sports and Exercise. 2004 Dec;36(12):2040-2045.
- Cyriax J. Textbook of orthopaedic medicine, diagnosis of soft tissue lesions, vol 1, 8th edition. London: Baillière Tindall; 1982.
- Ellsworth AA, Zoland MP, Tyler TF. Athletic pubalgia and associated rehabilitation. Int J Sports Phys Ther. 2014 Nov;9(6):774-84.
- Gomella P, Mufarrij P. Osteitis pubis: A rare cause of suprapubic pain. Rev Urol. 2017;19(3):156-163.
- Harøy J, Clarsen B, Wiger EG, et al. The Adductor Strengthening Programme prevents groin problems among male football players: a cluster-randomised controlled trial. Br J Sports Med. 2019;53(3):150-157.
- Harøy J, Thorborg K, Serner A, et al. Including the Copenhagen Adduction Exercise in the FIFA 11+ Provides Missing Eccentric Hip Adduction Strength Effect in Male Soccer Players: A Randomized Controlled Trial. Am J Sports Med. 2017;45(13):3052-3059.
- Hölmich P, Uhrskou P, Ulnits L, Kanstrup IL, Nielsen MB, Bjerg AM, Krogsgaard K. Effectiveness of active physical training as treatment for long-standing adductor-related groin pain in athletes: randomised trial. Lancet. 1999 Feb 6;353(9151):439-43.
- Ishøi L, Sørensen CN, Kaae NM, Jørgensen LB, Hölmich P, Serner A. Large eccentric strength increase using the Copenhagen Adduction exercise in football: A randomized controlled trial: Strength increase using Copenhagen Adduction. Scand J Med Sci Sports. 2016;26(11):1334-1342.
- Moreno-Pérez V, Travassos B, Calado A, Gonzalo-Skok O, Del Coso J, Mendez-Villanueva A. Adductor squeeze test and groin injuries in elite football players: A prospective study. Phys Ther Sport. 2019 May;37:54-59.
- Perez-Gomez, Jorge & Villafaina, Santos & Adsuar, Jose & Carlos-Vivas, Jorge & Garcia-Gordillo, Miguel & Collado-Mateo, Daniel. Copenhagen Adduction Exercise to Increase Eccentric Strength: A Systematic Review and Meta-Analysis. Applied Sciences. 2020.
- Rabe SB, Oliver GD. Athletic Pubalgia: Recognition, Treatment, and Prevention. Athletic Training & Sports Health Care. 2010;2(1):25-30.
- Silbernagel KG, Thomeé R, Eriksson BI, Karlsson J. Continued sports activity, using a pain-monitoring model, during rehabilitation in patients with Achilles tendinopathy: A randomized controlled study. The American Journal of Sports Medicine. 2007; 35(6):897-906.
- Serner A, Jakobsen MD, Andersen LL, Hölmich P, Sundstrup E, Thorborg K. EMG evaluation of hip adduction exercises for soccer players: implications for exercise selection in prevention and treatment of groin injuries. Br J Sports Med. 2014;48(14):1108-1114.
- Serner A, Weir A, Tol JL, Thorborg K, Lanzinger S, Otten R, Hölmich P. Return to Sport After Criteria-Based Rehabilitation of Acute Adductor Injuries in Male Athletes: A Prospective Cohort Study. Orthop J Sports Med. 2020 Jan 29;8(1):2325967119897247.
- Thorborg K, Reiman MP, Weir A, et al. Clinical Examination, Diagnostic Imaging, and Testing of Athletes With Groin Pain: An Evidence-Based Approach to Effective Management. J Orthop Sports Phys Ther. 2018;48(4):239-249.
- Weir A, Jansen JA, van de Port IG, Van de Sande HB, Tol JL, Backx FJ. Manual or exercise therapy for long-standing adductor-related groin pain: a randomised controlled clinical trial. Man Ther. 2011 Apr;16(2):148-54.
- Zuckerbraun BS, Cyr AR, Mauro CS. Groin Pain Syndrome Known as Sports Hernia: A Review. JAMA Surg. 2020 Apr 1;155(4):340-348.
