If you had to pick one injury to be good at treating what would it be?!
…A LATERAL ANKLE SPRAIN!!!!!
I remember in my physical therapy training, one of my professors stating that if you could treat a lateral ankle sprain, you could use variations on this theme to treat any other musculoskeletal foot or ankle injury.
“If you can treat an ankle sprain, you can treat any other foot or ankle injury”
Just as many experiences serve as reference frames, physical therapist’s (PTs) diagnosis and treatment of ankle sprains serves as a foundation on which to build when treating other foot and ankle pathologies.
From a physical therapy perspective, clinical practice guidelines (CPGs) can help inform treatment decisions because of their comprehensive and diligent efforts to distill up to date research and “best practices” based on clinical expertise. Just this year, an updated CPG on treating ankle sprains was released and motivated me to evaluate and revisit some of my treatment techniques for ankle sprains.
I was reminded of the importance of “getting back to basics” and wanted to share some of the recommendations and how I try to integrate these into my physical therapy practice in working with individuals who have experienced an ankle sprain.
The first step in evaluation and treatment decisions as guided by this CPG is the classification as either:
- “Acute Lateral Ankle Sprain”
- Injury within the past 72 hours
- With swelling, pain, or limited weight bearing tolerance
OR
- “Chronic Ankle Instability”
- History of prior ankle sprain(s) within the past 12 months with
- With history of instability and/or giving way
Since acute sprains are most common, I created the chart below summarizing the keys that I took away from the CPG recommendations for evaluation, prevention, and treatment for acute lateral ankle sprains:

Following the classification into an “Acute” or “Chronic” ankle injury, evidence recommends certain evaluation, prevention, and treatment techniques as described below.
Here is a chart distilling the findings and recommendations from the CPG for PTs (Ankle Sprains: What Updated Guidelines Mean for You):

Ankle Sprain Examination:
The main recommendations for examination after acute lateral ankle sprain are:
- Range of Motion (ROM) testing: closed chain dorsiflexion (lunge test)
- Strength of foot/ankle muscles
- Ankle joint mobility testing
- Weight bearing and jumping tolerance
- Balance testing (single leg stance and star excursion balance)
- Ankle ligament testing (see below)
A recommendation is made to use BOTH the Anterior Drawer Test (ADT) AND Reverse Anterolateral Drawer Test (ALDT) in examination of acute lateral ankle sprain. This is because up to 1/3 of ATFL tears can be missed by the anterior drawer test! (Li, 2020). The RALDT has been shown to have better accuracy to detect injury to the anterior talofibular ligament (ATFL), which is the most commonly injured ankle ligament (Li, 2020). ADT is performed in neutral ankle position while stabilizing the tibia and fibula and moving the talus, while the RALDT is performed in 10-15 degrees of plantarflexion (can palpate at lateral ligaments) and stabilizing the talus, while moving the tibia and fibula.
For test positions see the pictures below:


For chronic ankle instability (CAI), it is recommended to evaluate (in addition to tests previously mentioned):
- Single leg hopping, prior injury history (number of sprains), functional complaints, testing that mimics functional demands of daily living or sports as applicable
Ankle Sprain Prevention:
Prevention strategies are generally similar whether aiming to prevent an initial injury (“primary ankle sprain”) or subsequent ankle sprains (secondary, tertiary sprains). These include using external support (taping or bracing) (but NOT in isolation), balance and proprioception exercises, manual therapy and avoiding the use of ultrasound (see chart below):

Ankle Sprain Treatment:
Treatment for ankle sprains is very similar to prevention strategies and includes the use of:
- External support (taping or bracing) (but, not as stand-alone treatment!)
- Balance and proprioception exercises
- Neuromuscular retraining exercises
- Manual therapy (range of motion, stretching, joint mobilizations as necessary)
- Recommendation to NOT use ultrasound
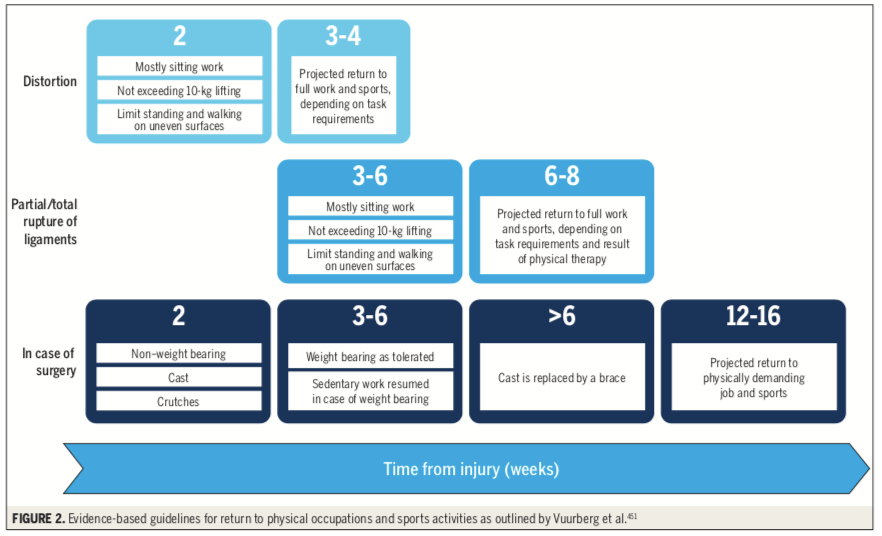
Ankle Sprain Prognosis:
Prognosis after ankle sprains is generally quite good and time to return to activity and sport is usually between 2-8 weeks depending on the severity of injury (see table below from CPG), but can take up to 3-4 months if surgical intervention is warranted:
I hope this has helped in how you may prioritize your evaluation and treatment techniques in physical therapy rehabilitation for individuals with lateral ankle sprains and chronic ankle instability.
References:
Patient Perspective from JOSPT Revised Ankle Sprain CPG:
Ankle Sprains: What Updated Guidelines Mean for You. J Orthop Sports Phys Ther. 2021 Apr;51(4):161.
Revised Ankle Sprain CPG (2021):
Martin RL, Davenport TE, Fraser JJ, Sawdon-Bea J, Carcia CR, Carroll LA, Kivlan BR, Carreira D. Ankle Stability and Movement Coordination Impairments: Lateral Ankle Ligament Sprains Revision 2021. J Orthop Sports Phys Ther. 2021 Apr;51(4):CPG1-CPG80.
Physical Therapist Perspective from JOSPT Revised Ankle Sprain CPG:
Physical Therapy After an Ankle Sprain: Using the Evidence to Guide Physical Therapist Practice. J Orthop Sports Phys Ther. 2021 Apr;51(4):159-160.
Li Q, Tu Y, Chen J, Shan J, Yung PS, Ling SK, Hua Y. Reverse anterolateral drawer test is more sensitive and accurate for diagnosing chronic anterior talofibular ligament injury. Knee Surg Sports Traumatol Arthrosc. 2020 Jan;28(1):55-62.
