Welcome to Part 2: Exercise Prescription for Lower Extremity Tendinopathy. If you missed Part 1 on Assessment check that out! Also, Part 3 on Individualizing Treatment to Patient Cases
Tendons, just like all the tissues in our body, feel different mechanical forces depending upon what movements we engage in (or not). In response to these loads, our body tissues (bone, muscles, tendons) are constantly remodeling. A key factor in preventing and recovering from tendon injuries (i.e., tendinopathies) is to optimize the load, or forces, felt at those tendons. In the beginning of treatment we usually “De-load” (aka activity restrict) and then progressively build load until the tendon can tolerate the amount of load needed to optimize function. As presented at the end of Part 1, the progression would look something like this:
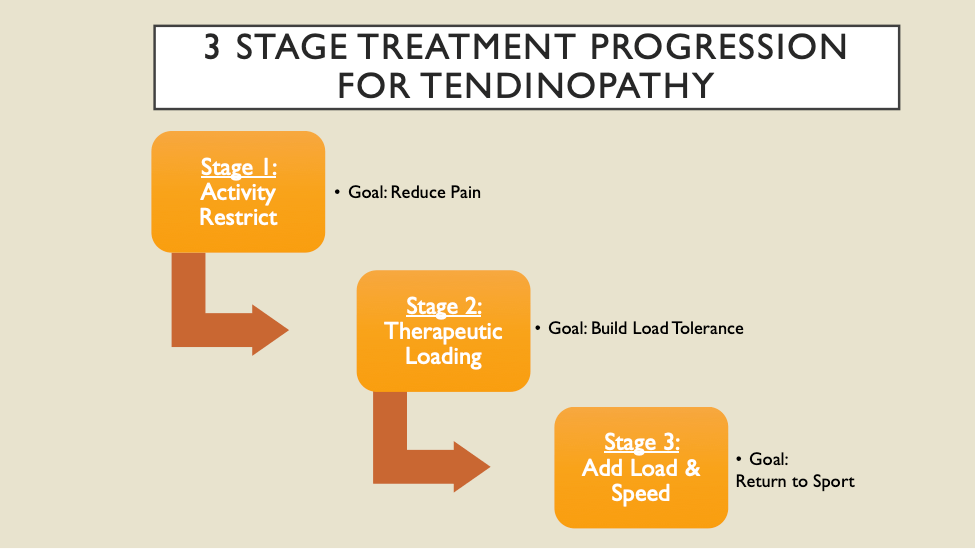
STAGE 1: Activity Restrict
If we remember that tendinopathies usually have an “overuse” or “overload” cause to them, it makes sense that some sort of activity restriction is usually necessary to allow that area to calm down. BUT, please do not mishear me and think that I am recommending staying away from ALL activity! We actually want our patients to be as active as they can be within a therapeutic range. Stopping ALL activity is usually not necessary and I have found that this fact alone can be very encouraging for patients who sometimes fear that they will be asked to stop running or sports activities entirely. One study looking at patients with Achilles’ tendinopathies, showed that long-term (3,6, 12 months) improvements in function and pain were the same for a group that rested completely for 6 weeks before beginning a progressive loading program and a group who continued being active for that first 6 weeks (as long as they followed a “pain monitoring model” (i.e., were not active to the point of causing pain > 5/10 and any pain brought on by activity went away by the following morning)1. Currently, I use this pain monitoring model1, 2 with patients, though I typically use a more conservative pain threshold and try to keep patients at < 3/10 pain.

A great visual when thinking about hitting this “sweet spot” of loading not too much…not too little…just right…is the “Envelope of Function” as coined by Dr. Scott Dye3. An important component of this paradigm is that a tissue’s load tolerance will be reduced after injury (e.g., a pathological tendon won’t be able to tolerate as much load intensity or frequency as a healthy tendon) but will still have the ability to take on some loading. See Figure Below for this concept as applied to an ACL injury/recovery (the threshold for physiologic tissue overload is represented with the dark black line. You can watch it decrease immediately following injury and increase with progressive, careful rehabilitation across the four pictures).
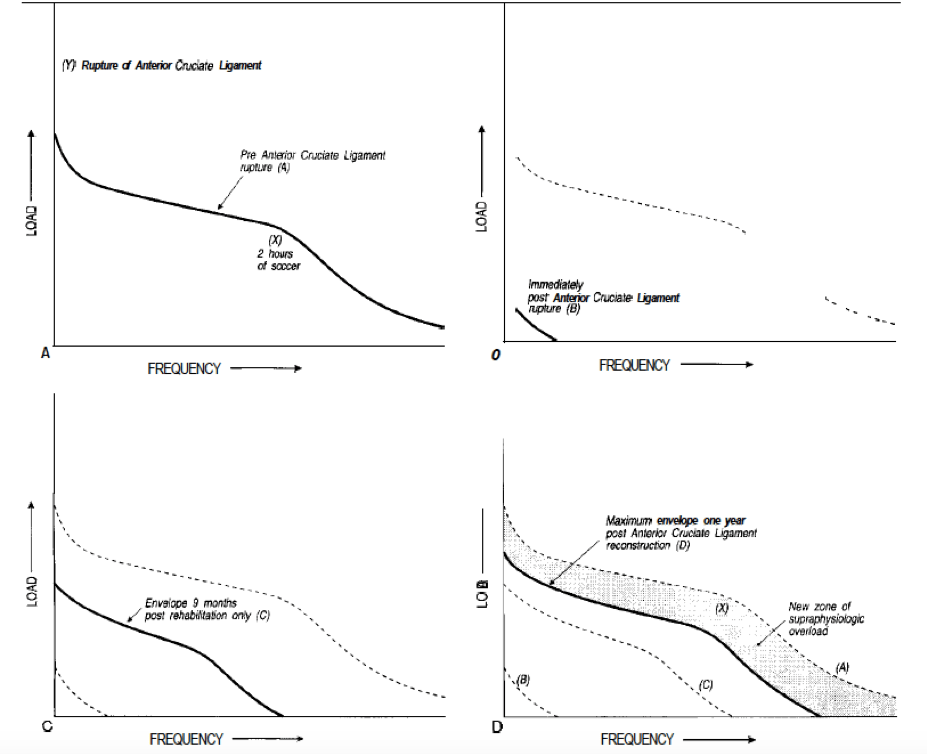 (Dye, 1996)3
(Dye, 1996)3
Even though I believe that the long-term success of tendinopathy rehabilitation will be built on loading prescription, this first stage of treatment is also where your adjunct treatments for pain and protecting the tendon’s end range excursion can be useful4. As part of protecting the tendon, I would recommend refraining from stretching in this phase in order to avoid symptom provocation.
Adjunct treatments to loading/exercise prescription may include:
- Icing and NSAIDS
- Achilles’ Tendinopathy: heel wedge, or wearing shoes with higher heel (avoid zero drop) to reduce stretching into extremes of dorsiflexion
- Posterior Tibialis Tendinopathy: taping or orthotics supporting the longitudinal arch
- Plantar Fasciitis: taping or orthotics supporting the longitudinal arch
- Patellar Tendinopathy: taping or bracing
- Gluteal Tendinopathy: walking stick or cane to reduce load in single limb support during walking
- High Hamstring Tendinopathy: using a seat cushion or donut pad to reduce ischial tuberosity pain/irritation and walking with shorter strides to reduce stretch
*A Note on Manual Therapy:
-
- Anecdotally, some form of soft tissue mobilization can be very effective in progressing these patients from a “chronic” type issue into seeing some real improvements in function. Whether this is due to kickstarting the inflammatory response via more aggressive instrument assisted techniques, or whether the hands-on treatments improve blood flow and/or sensory signaling (introduce non-painful sensory stimuli) I am not sure. However, patients seem to respond well to this treatment (they report improvements in pain and subjectively it seems to help at least in the first 1-3 weeks of treatment).
STAGE 2: Therapeutic Loading
As we load tendons, we must consider the patient’s level of irritability or acuity. Then, we can use the “FITT” principles of loading (Frequency, Intensity, Time, and Type) to prescribe exercises and optimize load at the tendon. Finally, there will naturally need to be some trial and error as you adjust loading parameters based on the patient’s response and progress volume, magnitude, and finally rate of loading.
With the goal of loading in a therapeutic range for the patient: here are three keys to exercise prescription for tendinopathy:

1st: Stage Based on Symptom Irritability
In the beginning of your treatment (with information gathered from your evaluation), it is helpful to stage your patient based on their tolerance to loading. This approach to treatment has been used for low back pain5 and neck pain6 and has been proposed as clinically useful in guiding treatment for shoulder pain7. In order to assess the irritability of the tendon in question, it is helpful to get in the habit of rating these different variables (related to pain and symptom presentation):
- How bad is the pain with a loading movement specific to that tendon? (e.g., single leg calf raise for Achilles’ tendinopathy)
- When is the onset of pain in relation to activity/loading?
- How long does the pain last after activity/loading?
- What activities is the individual limited in doing?
Then, you can start to get a sense for what treatments and FITT variables will be most appropriate for the patient. To stage based on symptom irritability, try to best fit these categories:
| Low Irritability
(High Load Tolerance) |
Moderate Irritability
(Medium Load Tolerance) |
High Irritability
(Low Load Tolerance) |
| Pain ≤ 3/10 | Pain = 4-7/10 | Pain > 7/10 |
| Pain begins well into the activity
(e.g., after 5 miles of running) |
Pain at the beginning of activity, but decreases once tendon “warms up” | Pain at the beginning of activity that does not decrease with warm up |
| Pain does NOT last after activity | Pain stops 1-2 hours after activity | Pain LASTS > 1-2 hours after activity |
| Pain/symptoms are more “bothersome” than limiting, though may limit higher level athletic performance- such as longer or faster running efforts, jumping, or full force kicking | Pain/symptoms that interfere with recreational activities, can still engage in most daily movements with no symptoms | Pain/symptoms with low level activities such as walking, activities of daily living
*Sitting may be painful *walking/standing/sleeping may be affected |
2nd: Optimize Load
As mentioned above, tendons need appropriate loading in order to be healthy and continue to remodel in adaptive ways. Here are some recommended parameters for exercises4, 9,10, 11, 12.
FREQUENCY:
- Minimum Frequency: 3-4x/week
- Maximum Frequency: every day (I do not recommend multiple times a day for treatment as long as the patient is able to complete all exercises in one session; remember we are dealing with an “overuse” or “overload” injury)
- Tendons need time to recover to promote positive adaptations (similar to muscle): one study looking at net collagen synthesis in tendons following a bout of exercise noted that net collagen synthesis was higher at 36-72 hours following exercise8. This suggests the need for a recovery period to optimize structural adaptations in tendons following a bout of exercise (see figure below):
 (Magnussen, 2010)8
(Magnussen, 2010)8
INTENSITY:
- Minimum Intensity: enough to get the muscle to contract and feel load at the tendon but not aggravate or provoke symptoms (can be as low as a sub maximal isometric contraction, contracting at 25-50% of max contraction, but ideally progressing to 65% of maximum voluntary contraction)
- Maximum Intensity/Strength Goals: ultimately, there should be build up in weight and intensity, more on these specific “strength” goals in Part 3. This could look like building up to performing single leg calf raises with #35-55 for Achilles’ tendinopathy.
TIME:
Time of loading is mostly dictated by your sets and repetitions prescribed for loading as well as frequency throughout the week (see Frequency). Research suggests that heavy slow resistance exercises and reduced frequency (e.g., 3x/week) can be just as effective as training every day with eccentrics only!12
- Minimum Time: Early on 5-6 sets of 30 second isometric holds (with 1-2 min rest between sets, this could take about 8-10 minutes).
- Maximum Time: Later, when performing combined concentric/eccentrics for 3 sets of 8-15 repetitions and with multiple exercises, this could take 20-30 minutes. (I will usually start with higher rep scheme/lower weight 3×15 and progress to loaded 3×8, or even 4×6-8 repetitions).
TYPE:
- Isometrics Early: isometrics allow you to load the muscle-tendon unit in a way that often is more tolerable (less painful) than moving through range, I start here with the majority of the patients that I see with tendinopathy
- Some research data in patellar tendinopathy indicates isometrics may have an analgesic effect13, 14, 15 (However, we need more data on this!)
- Progress to Combined Concentrics/Eccentrics: Traditional tendinopathy loading programs in the lower extremity have emphasized eccentric loading11. But, newer approaches have shown positive outcomes on pain and function with heavy slow resistance training using reduced time and frequency of loading and a combination of concentric and eccentric loading12.
3rd: Progress Load
Progression of load can be achieved by changing any of these variables (Frequency, Intensity, Time, Type) of exercise prescription. Some progressions will happen early in the rehabilitation process, for example I will transition patients from isometrics to combined concentric/eccentric exercises as quickly as they are able to tolerate it (pain <3/10). Other progressions will take more time (e.g., adding magnitude/weight to exercise and introducing a higher rate of loading).
I will discuss these progressions more as they apply to the patient case examples in Part 3! Also, progressing load and adding speed to loading signal that we are moving into Stage 3 of rehabilitation for these tendinopathies.
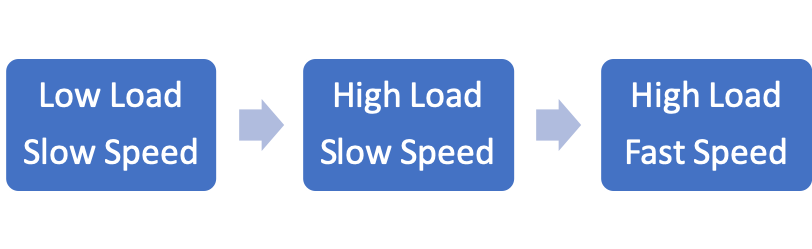
STAGE 3: Add Load & Speed
The basic idea here is to gradually add load and speed (adding volume or magnitude of load first and then progressing to faster loading rates):
This will become more tangible with the patient case examples in Part 3. Also, much of this stage should be pretty similar to other orthopedic physical therapy rehabilitation methods where the goals are to:
- Increase strength and mobility
- Increase complexity of movements
- Train functional movement patterns
*Note here that RATE of loading is one of the last things to increase!
Also, in Part 3: some notes on return to sport and return to run progressions.
Check out Part 3 of this series with Patient Case Examples and applications of these principles!
References for Part 2:
- Silbernagel KG, Thomeé R, Eriksson BI, Karlsson J. Continued sports activity, using a pain-monitoring model, during rehabilitation in patients with Achilles tendinopathy: A randomized controlled study. The American Journal of Sports Medicine. 2007; 35(6):897-906.
- Silbernagel KG, Thomeé R, Thomeé P, Karlsson J. Eccentric overload training for patients with chronic Achilles tendon pain—a randomized controlled study with reliability testing of the evaluation methods. Scand J Med Sci Sports. 2001; 11:197-206.
- Dye SF. The knee as a biologic transmission with an envelope of function: a theory. Clinical orthopaedics and related research. 1996; 325:10–18.
- Malliaras P. Mastering Lower Limb Tendinopathy 2nd https://www.tendinopathyrehab.com/ Accessed: December 18th, 2018
- Fritz JM, Cleland JA, Childs JD. Subgrouping Patients With Low Back Pain: Evolution of a Classification Approach to Physical Therapy. Journal of Orthopaedic & Sports Physical Therapy. 2007;37(6):290-302.
- Childs JD, Cleland JA, Elliott JM, et al. Neck Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health From the Orthopaedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008;38(9):A1-A34.
- McClure PW, Michener LA. Staged Approach for Rehabilitation Classification: Shoulder Disorders (STAR-Shoulder). Physical Therapy. 2015;95(5):791-800.
- Magnusson SP, Langberg H, Kjaer M. The pathogenesis of tendinopathy: balancing the response to loading. Nature Reviews Rheumatology. 2010; 6(5): p. 262-268.
- Malliaras P, Barton CJ, Reeves ND, Langberg H. Achilles and Patellar Tendinopathy Loading Programmes: A Systematic Review Comparing Clinical Outcomes and Identifying Potential Mechanisms for Effectiveness. Sports Medicine. 2013;43(4):267-286.
- Malliaras DP, Purdam C. Rehabilitation of lower limb tendinopathy. In Touch. 2014;(149):7.
- Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Heavy-Load Eccentric Calf Muscle Training For the Treatment of Chronic Achilles Tendinosis. The American Journal of Sports Medicine. 1998;26(3):360-366.
- Beyer R, Kongsgaard M, Hougs Kjær B, Øhlenschlæger T, Kjær M, Magnusson SP. Heavy Slow Resistance Versus Eccentric Training as Treatment for Achilles Tendinopathy: A Randomized Controlled Trial. The American Journal of Sports Medicine. 2015;43(7):1704-1711.
- Rio E, Kidgell D, Moseley L, Pearce A, Gaida J, Cook J. Exercise to reduce tendon pain: A comparison of isometric and isotonic muscle contractions and effects on pain, cortical inhibition and muscle strength. Journal of Science and Medicine in Sport. 2013;16:e28.
- Rio E, Kidgell D, Purdam C, et al. Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. British Journal of Sports Medicine. 2015;49(19):1277-1283.
- Rio E, van Ark M, Docking S, et al. Isometric Contractions Are More Analgesic Than Isotonic Contractions for Patellar Tendon Pain: An In-Season Randomized Clinical Trial. Clin J Sport Med. 2017;27(3):7.

11 Comments Add yours