Prescribing exercise in physical therapy is almost a given. As physical therapists, our profession encourages us to describe ourselves as “Movement Experts”. Furthermore, despite there being a current “movement” (see what I did there?!) to broaden the scope outside of just exercise–related movement, for the majority of our patients (e.g., incorporating regular small bouts of movement throughout the day), exercise is going to make up the majority of their daily “movement diet”.
So, how can we OPTIMIZE the results that we are getting from the exercise prescriptions (Rxs) we are making in physical therapy (PT)?
Here are 3 simple ways to guide your PT Exercise Prescriptions:
(Answering the “Why” “What” and “How Much” questions most effectively!)
- Define WHERE YOU ARE GOING > (the patient’s “WHY”)
- Choose the TYPE of exercise wisely > (define the “WHAT”)
- Avoid Extremes (under loading OR over loading) > (Decide “HOW MUCH”)
- Define WHERE YOU ARE GOING (WHY EXERCISE?):
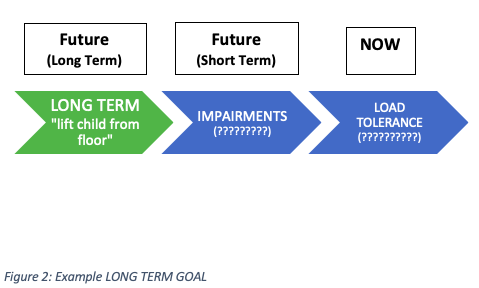
The first step in this process is to engage your patient in why they are in physical therapy in the first place (i.e., why do PT exercises at all?!). What is the highest priority LONG-TERM GOAL of your patient? This goal should be the end point of formal physical therapy treatment.

Let’s use a hypothetical case example to illustrate these exercise prescription principles. Let’s say I am working with a 27-year-old male with “nonspecific” low back pain in a physical therapy setting. Fred has had different episodes over the past three years where he has “tweaked” his back picking up objects from the floor (has no red flag symptoms or significant past medical history).
Fred’s main goal from physical therapy is this:
“I want to be able to pick up my 6-month-old daughter without worrying about my back hurting”
How does this fit into our progress? See below:
2. Choose the TYPE of exercise wisely (WHAT KIND OF EXERCISE?)
The next step in the process is to identify the specifics that are standing in your patient’s way from attaining their long-term goal. I like to think about these things as the “low hanging fruit” that show up in your clinical examination with the patient. We commonly refer to these as “impairments” such as: Weakness, reduced range of motion, inflexibility, poor motor control, pain, reduced balance or proprioception, sensory deficits…
*Quick note: I am careful in communicating with patients regarding these treatable skills and building blocks of movement. In the spirit of not projecting overly “nocebo” laced language (i.e. “impairments”), I try to use terms such as “areas for growth” or “skills to practice”.
These areas for growth that you pick up on in your comprehensive physical therapy examination, guide the TYPE of exercises that you will prescribe. Again, back to Fred and wanting to help him out: in his physical therapy examination, when Fred bends forward and returns to standing he has limited motion and after five toe touches starts to walk his hands up his legs for support (also starts complaining of pain/discomfort at his low back). When asked to do a squat motion, he rounds his back and tucks his pelvis under to perform this motion. Exam findings may suggest that Fred has some movement patterns that may not be ideal. He has a hard time with pain-free forward bending (combined lumbar and hip flexion) and hip hinging (controlled hip flexion in squatting), let’s call this: “poor lumbopelvic dissociation”. Now we have identified a skill that we might train (i.e., “Impairment”) to try to improve his long-term goal. See Below:

Again, the type of exercise that you prescribe will be matched on the goal of what skill you are trying to train or area you are trying to treat. This overlaps a little bit with the section below discussing load tolerance, but for the sake of simplicity we can think about defining the type of exercise based on the category of skill that you are trying to train. See Chart Below:

We also want to think about getting more specific or nuanced with our exercise prescriptions and defining a specific exercise (e.g., squat vs. knee extension) to train, what type of muscle contraction, total volume of training, and frequency. I will address many of these parameters in the next section, but a quick word on specific exercise selected and type of muscle contraction:
This will depend largely again on your GOAL for the exercise. There are a myriad of specific exercises to choose from that may enhance movement. It is beyond the scope of this post to dig into this too deeply, but suffice it to say that the decision to perform a squat vs. knee extension exercise should be based on some sort of rationale towards attaining your long-term goal (is this goal leg strength? Range of motion? functional movement pattern training like sit to stand?, etc.). Also, the type of muscle contraction selected can be different depending on your goal, type of injury, and acuity of the injury. For example, isometric exercises may be a nice choice early in injury recovery as they are often better tolerated and there is some research to suggest that they may be analgesic (Rio, 2015; Rio 2017).
Eccentric exercises may be beneficial for upper limb and lower limb tendinopathies (Alfredson, 1998; Beyer, 2015; Croisser, 2007; Tyler, 2010;), (see this post for a more in depth discussion of exercise prescription for lower limb tendinopathies: “Exercise Prescription for Lower Extremity Tendinopathies”). Also, there has been research to support the importance of eccentric (lengthening) exercises to reduce the risk of reinjury in hamstring muscle strains (Hickey et al., 2020). It may be useful to remember, however, that a healthy muscle should be able to engage in each of these types of contraction without pain (isometric, eccentric, and concentric contractions).
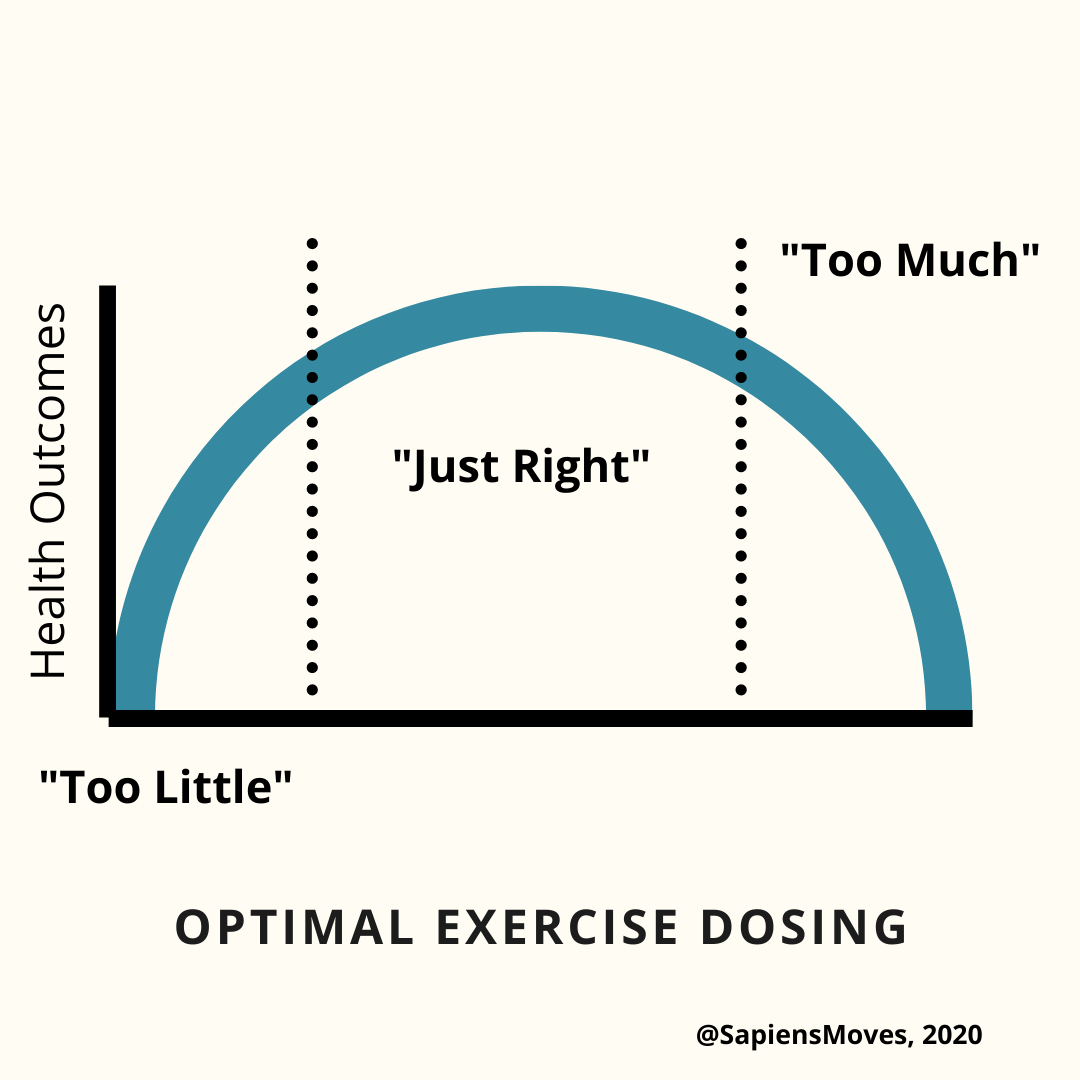
3. Avoid Extremes (under loading OR over loading) (HOW MUCH EXERCISE?)
The third step in choosing appropriate exercise for your patients is dosing, or “HOW MUCH” exercise is appropriate. This is perhaps the most nuanced part of the puzzle, and there are no perfect answers. However, in order to have a place to start it is helpful to be able to have a baseline assessment. This baseline assessment has been described in different terms, but my favorite are “Load Tolerance” and “Tissue Capacity”, because I think they really get at what we are after: “How much force or load can the patient and/or the tissue of interest handle RIGHT NOW!” For a great editorial on defining the term “Tissue Capacity” see this paper from Dr. Jill Cook and Dr. Sean Docking: Defining Tissue Capacity (Cook & Docking, 2015)
For our patient, Fred, we know that his “tolerance” to loading right now is: five toe touches before he starts to walk his hands up his legs for support and has an onset of low back pain.

Because we want to work on his lumbopelvic control, we teach him to “hip hinge” with a dowel and progress that into teaching him to squat and deadlift. We will use no weight to start and progressively add weight, a similar progression may be seen with his sets and reps and we may start him with a 2-3 day per week strength program once we are able to add weight to these movements. Also, we must remember that MORE is not always better! A recent study showed increased training frequency (6 days per week vs. 3 days per week) did not lead to improved hypertrophy/strength (as long as training volume was kept equal) (Colquhoun, 2018).
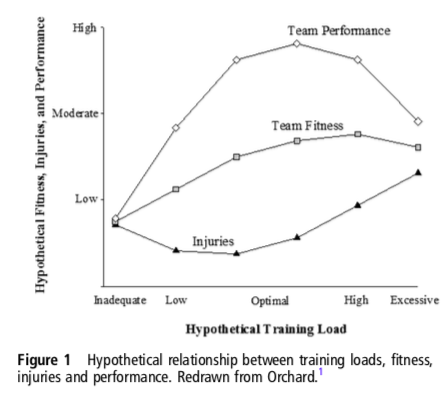
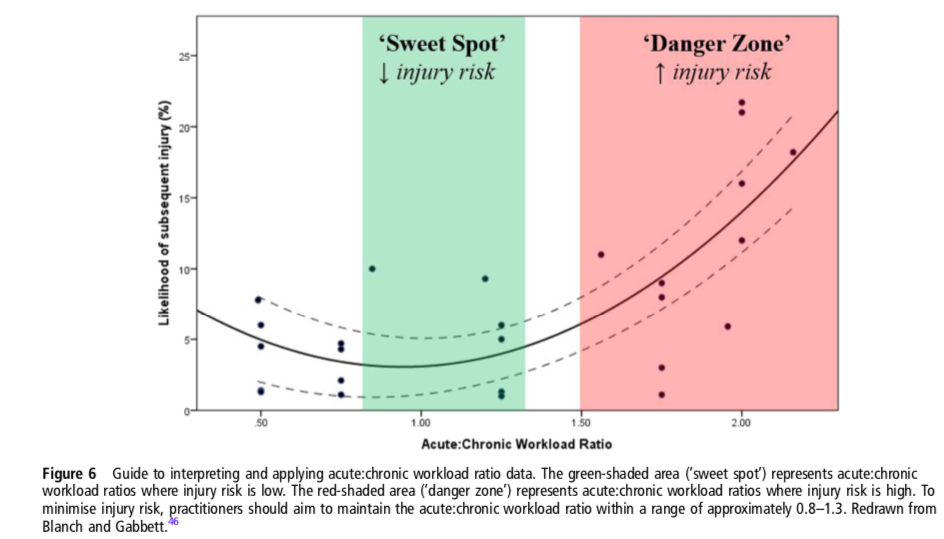
In order to evaluate your patients CURRENT LOAD TOLERANCE (related to prior fitness capacity and current fitness)? You may utilize subjective complaints of pain, objective movement assessment and strength/endurance testing and even may utilize an objective measure such as Acute to Chronic workload ratio to gauge their capacity based on current and past training volumes (Gabbett, 2016). All of these things can help you attain the “sweet spot” of dosing so that you are optimizing performance and reducing injury risk (see graphs below from Gabbett, 2016):
Optimizing Performance with Training Load:
Reducing Injury Risk with Training Load:
I find that the analogy of exercise as medicine can be useful. Picture a pill bottle: you have dosing parameters: how much active ingredient is contained in each pill, recommended dosing quantity (how many pills) and frequency (how many times per day, week, month) for a recommended result (reduce pain, swelling, inflammation). There are multiple types of pills that you may take for the same condition and your best choice will be based on your patient’s individual situation (age, medical history and comorbidities, goals, etc.)
The sets, reps, intensity, and frequency that you choose will be dependent on your exercise GOAL (see chart above). For example, we know that strength gains will necessitate a certain set/rep/intensity scheme. For a nice discussion of “dosing” exercise and a reinforcement of some of the principles that I have discussed above, check out this great podcast discussion “Think Before You 3×10”.
A simplified schematic for exercise dosing/volume is shown below:
Final Thoughts on Exercise Prescription:
Exercise sets, reps, rest and total load are important, but there is MUCH more to prescribing exercise than just these parameters…
I hope that this post has given you a chance to reflect on how and why you prescribe the exercises that you do in physical therapy. The purpose of this discussion on exercise prescriptions is not to overwhelm you with variables, but instead to help you to become more intentional about the factors that go into your exercise recommendations.
References:
- Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Heavy-Load Eccentric Calf Muscle Training for the Treatment of Chronic Achilles Tendinosis. The American Journal of Sports Medicine. 1998;26(3):360-366.
- Beyer R, Kongsgaard M, Hougs Kjær B, Øhlenschlæger T, Kjær M, Magnusson SP. Heavy Slow Resistance Versus Eccentric Training as Treatment for Achilles Tendinopathy: A Randomized Controlled Trial. The American Journal of Sports Medicine. 2015;43(7):1704-1711.
- Colquhoun RJ, Gai CM, Aguilar D, et al. Training Volume, Not Frequency, Indicative of Maximal Strength Adaptations to Resistance Training: Journal of Strength and Conditioning Research. 2018;32(5):1207-1213.
- Cook J, Docking S. “Rehabilitation will increase the ‘capacity’ of your …insert musculoskeletal tissue here….” Defining ‘tissue capacity’: a core concept for clinicians. Br J Sports Med. 2015;49(23):1484-1485.
- Croisier JL, Foidart-Dessalle M, Tinant F, Crielaard JM, Forthomme B. An isokinetic eccentric programme for the management of chronic lateral epicondylar tendinopathy. British Journal of Sports Medicine. 2007;41(4):269-275.
- Gabbett TJ. The training—injury prevention paradox: should athletes be training smarter and harder? British Journal of Sports Medicine. 2016;50(5):273-280.
- Hickey JT, Timmins RG, Maniar N, et al. Pain-Free Versus Pain-Threshold Rehabilitation Following Acute Hamstring Strain Injury: A Randomized Controlled Trial. J Orthop Sports Phys Ther. 2020;50(2):91-103.
- Rio E, Kidgell D, Purdam C, et al. Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. British Journal of Sports Medicine. 2015;49(19):1277-1283.
- Rio E, van Ark M, Docking S, et al. Isometric Contractions Are More Analgesic Than Isotonic Contractions for Patellar Tendon Pain: An In-Season Randomized Clinical Trial. Clin J Sport Med. 2017;27(3):7.
- Tyler TF, Thomas GC, Nicholas SJ, McHugh MP. Addition of isolated wrist extensor eccentric exercise to standard treatment for chronic lateral epicondylosis: A prospective randomized trial. Journal of Shoulder and Elbow Surgery. 2010;19(6):917-922.
- https://evidenceinmotion.com/clinical-podcast-think-before-you-3×10-dr-neil-sheth/

One Comment Add yours