KNEE “STIFFNESS” AFTER TKA:
One of the common issues that I see a lot in my physical therapy work with patients is addressing pain and stiffness after knee replacement surgery. Patients are sometimes surprised at how much time it takes to regain adequate range of motion on their post-operative knee and this is one of our first goals in therapy as it greatly impacts their functional mobility (e.g., walking, getting up from a chair, etc.).
In some cases, patients attending physical therapy after having a total knee replacement (aka “Total Knee Arthroplasty”, TKA) will continue to have “stiffness” in their joint that persists despite interventions that aim to increase range of motion of the post-surgical knee joint. If this stiffness severely limits or impacts function, or if a patient falls below a set level of acceptable range of motion, a procedure called a “Manipulation Under Anesthesia (MUA)” can be performed by an orthopedic surgeon as a more aggressive measure to regain knee motion (usually used to increase flexion, less commonly used to improve extension) (Kornuijt, 2018). It has been reported that about 1.3-13.5% of those undergoing TKA may require an MUA to restore knee range of motion (Kornuijt, 2018).
Though there is not a standard amount of “adequate” knee range of motion following TKA surgery, one proposed cutoff is that patients should achieve 0 to 110 degrees of knee flexion range of motion (obtaining full extension or straightening of the joint and able to bend the knee 110 degrees) (Kornuijt, 2018). Recommendations on how early a patient should be able to obtain this range of motion vary based on the surgeon. However, most agree that patients should be at this level within 12 weeks (3 months) after surgery.
A manipulation under anesthesia (MUA) may be indicated if patients are limited to less than 90-95 degrees of knee flexion (bending) (or unsatisfactory range of motion impacting function). Surgeons vary based on when in the post-operative time line they will elect to perform a MUA; some performing this procedure within 1-6 weeks of the TKA surgery (“Early MUA”) and some performing within the 6-12 week post-operative time frame (“Late MUA”). There is no consensus on whether “Early” vs. “Late” MUA has superior outcomes; though outcomes do seem to be better if MUA is performed within 12 weeks post-operatively (within the first 12 weeks following surgery) (Isaa, 2014).
OUTCOMES AFTER MANIPULATION UNDER ANESTHESIA FOLLOWING TKA:
Following a MUA, patients on average will regain 30 degrees of flexion and 5 degrees of extension range of motion (Kornuijt, 2018); Gu, 2018; Fitzsimmons, 2010; Ghani, 2012). One systematic review of 22 studies, reported an average of 32 degrees of flexion gained and 36 degrees of total range of motion gained after MUA (Gu, 2018).
Generally, MUA is effective to improve range of motion after TKA. In one systematic review, all 22 studies reviewed showed that:
Patients undergoing a manipulation after knee replacement had significant increases in flexion range of motion after the manipulation procedure (Gu, 2018)
Rehabilitation following an MUA is not standardized and has not been widely studied. However, most clinical recommendations include intensive physical therapy that includes passive range of motion, active assisted range of motion, and in some cases the use of continuous passive motion machines to sustain as much of the knee motion gained during the manipulation procedure as possible.
If MUA does not restore adequate motion, further surgical interventions may be indicated such as an arthroscopic debridement (e.g., removing scar tissue surgically) and in some cases a second or third MUA may be indicated.
RISK FACTORS FOR DEVELOPING KNEE “STIFFNESS” AFTER TKA:
Even though we do not know for sure the exact cause of “stiffness” in some individuals after TKA surgery (most suggest it is due to increased fibrosis or scar tissue formation, but there is not a consensus as to why this occurs in some), there are certain factors that can increase risk of having reduced knee range of motion. One study found three specific risk factors that were significant; Patients with these risk factors (in retrospective analysis) were more likely to develop stiffness requiring MUA procedures. The factors that increased risk were (Newman, 2018).
- Younger Age (average 55 years of age vs. “older” TKA patients averaging 65 years of age)
- Current Smoker
- History of prior knee surgery
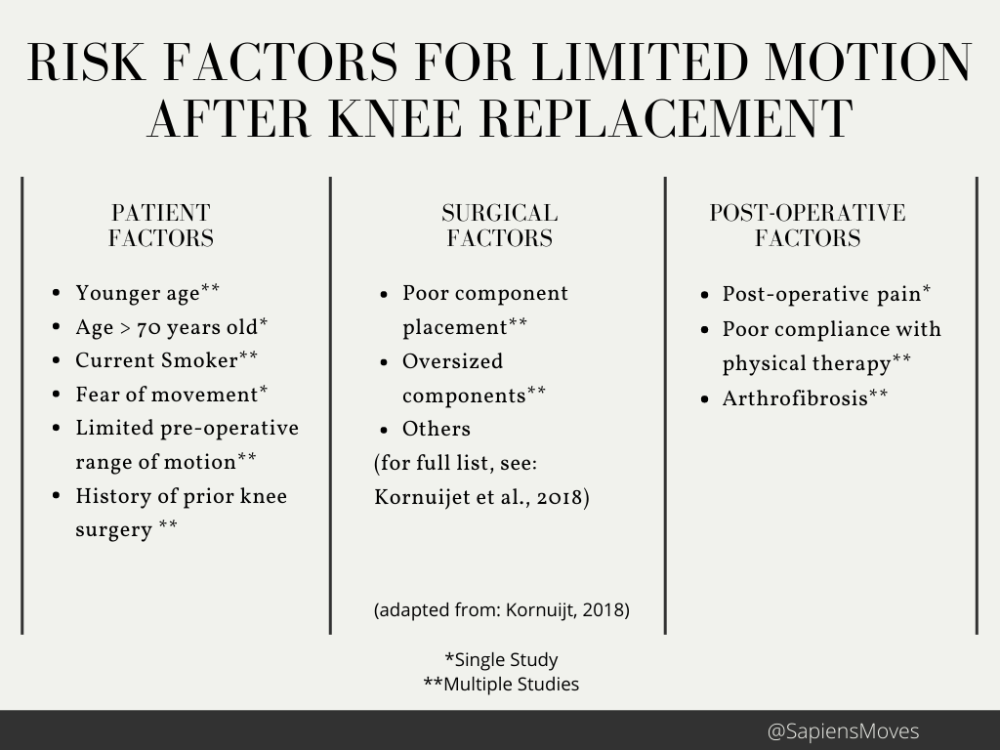
Another study exploring risk factors that may increase likelihood of “stiffness” after TKA performed a narrative review of the literature and reported on both patient and surgical risk factors (See table below for a summary of adapted results from this review):
I hope this post has helped inform realistic expectations for regaining range of motion following knee replacement surgery and when a manipulation under anesthesia may be indicated.
Remember, “MOTION IS LOTION” and good luck regaining that knee motion after surgery!
REFERENCES:
- Fitzsimmons SE, Vazquez EA, Bronson MJ. How to Treat the Stiff Total Knee Arthroplasty?: A Systematic Review. Clin Orthop Relat Res. 2010;468(4):1096-1106.
- Ghani H, Maffulli N, Khanduja V. Management of stiffness following total knee arthroplasty: A systematic review. The Knee. 2012;19(6):751-759.
- Gu A, Michalak AJ, Cohen JS, Almeida ND, McLawhorn AS, Sculco PK. Efficacy of Manipulation Under Anesthesia for Stiffness Following Total Knee Arthroplasty: A Systematic Review. The Journal of Arthroplasty. 2018;33(5):1598-1605.
- Issa K, Banerjee S, Kester MA, Khanuja HS, Delanois RE, Mont MA. The Effect of Timing of Manipulation Under Anesthesia to Improve Range of Motion and Functional Outcomes Following Total Knee Arthroplasty: The Journal of Bone and Joint Surgery. 2014;96(16):1349-1357.
- Kornuijt A, Das D, Sijbesma T, de Vries L, van der Weegen W. Manipulation under anesthesia following total knee arthroplasty: a comprehensive review of literature. Musculoskelet Surg. 2018;102(3):223-230.
- Newman ET, Herschmiller TA, Attarian DE, Vail TP, Bolognesi MP, Wellman SS. Risk Factors, Outcomes, and Timing of Manipulation Under Anesthesia After Total Knee Arthroplasty. The Journal of Arthroplasty. 2018;33(1):245-249.
