A runner who has suffered a bone stress injury will likely have one question front and center in their mind: “When can I get back to running?” To answer this question, there are some factors that can help predict a realistic healing timeline and inform injury prognosis after bone stress injuries (BSIs). Knowing what factors to focus on can be helpful in reducing risk of reinjury and optimizing bone healing as someone reintroduces activity.
The timing and guidelines offered below should not be used in place of professional medical advice and it is important to note that there is high individual variability in time course of these injuries. Monitoring clinical findings throughout progression of rehabilitation cannot be understated and tips on this will be discussed more below. As one Physical Therapist advises:
“Treat the Patient, Not the X-Ray”
(Warden, 2014)
Ok, but what does this mean in terms of getting back to running?! Evidence suggests that return to sport (i.e., running) time frames are best predicted on the severity of the bone stress injury as classified by 2 factors (Dobrindt, 2012; Kahanov, 2015; Liem, 2013; Tenforde, 2016):
- Location of injury (i.e., “High-Risk” vs. “Low-Risk” site)
- “Grade” of injury based on MRI findings
For a more comprehensive discussion of classifications of bone stress injuries, please see Part 1: Classifying “Bone Stress Injuries” and Tips for Prevention
The overall progression of rehabilitation after Bone Stress Injuries can be simplified into 3 Phases:
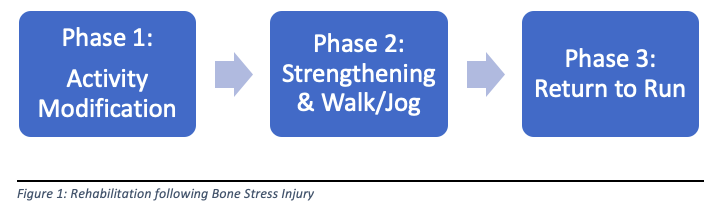
Phase 1: Activity Modification & Early Rehabilitation
To allow for bone healing after a BSI, it is often necessary to remove or reduce weight bearing on the lower extremity that has been injured. Return to full weight bearing activities for most bone stress injuries will be possible after 4-6 weeks, though BSIs in some locations may need closer to 8-12 weeks (Kahanov, 2015).During the initial phase of treatment, “High risk” sites of BSI are usually immobilized in a cast or walking boot and patients are “Non-weight bearing” on that limb; utilizing crutches or another form of assistive device (Liem, 2013). This recommendation for “Non-weightbearing” early on after injury also holds true for higher “Grades” of injury, especially stress fractures. Individuals with BSIs at “Low risk” sites or with lower “Grades” of injury (e.g., “stress reaction”) are usually given partial weight bearing ability, but still often utilize some sort of external device to reduce loading, such as a walking boot or stiff orthotic (Liem, 2013).
See Table Below for Rough Times for General Guidelines for Return to Weight Bearing:

Remember that if the BSI is a stress fracture, the time frames listed above will likely be periods of “Non-Weight Bearing” for lower grade BSIs these may be periods of “Weight Bearing as Tolerated” or “Partial Weight Bearing”.
During this initial phase, aerobic conditioning can be maintained with non-weight bearing forms of exercise including aqua jogging, upper limb ergometry, and in some cases stationary bicycle, elliptical, and Anti-gravity treadmill training. Also, some types of lower limb strengthening may be appropriate depending on the site of injury and pain provocation with exercises. This will vary greatly and is best assessed with clinical findings in conjunction with location and “grade” of injury.
Phase 2: Strengthening & Walk/Jog
After the initial phase of reduced loading and activity modification, it is necessary to progress strengthening of the leg muscles and start to reintroduce higher amounts of loading volume at the bone. As discussed in the first post on this topic, with increases in loading, whether that be by increasing walking distance, increasing weight for a squat exercise, or starting early bouts of jogging we must be careful to allow for adequate tissue (bone) recovery.
As I prescribe exercise to individuals in this stage of recovery, I will often utilize a 1 day of exercise followed by 1 day of recovery schema. With each subsequent day of exercise, or at least over the course of a week (roughly 3-4 “loading sessions”) my goal is to gradually build up volume of load- either by gradually increasing weight or repetitions of an exercise. How quickly and if progression of load is appropriate following a recovery day will depend on the individual’s muscle soreness and if any pain or swelling is present. I find pain a very useful clinical indicator of load tolerance and as applied to bone stress injury- my tolerance of pain as a response to loading is strict: I want to see NO PAIN DURING OR AFTER EXERCISES! An analogy to this may be the idea of monitoring swelling and soreness in patients after knee surgery. One algorithm for progression or regression of exercises based on soreness and swelling has been called “soreness rules” and dictates regression or maintaining load if soreness (or swelling) is present during or after training sessions and allows for progression of load if there is no increase in symptoms (swelling or soreness) during or after training (APTA Current Concepts of Orthopaedics).
Pain monitoring for BSIs or following knee injuries may be different than utilizing pain monitoring for tendinopathy rehabilitation in which some mild levels of pain (< 3/10) are tolerable and may be expected (See this blog post for a more comprehensive discussion of pain monitoring: Exercise Prescription for Lower Extremity Tendinopathy Also, two excellent articles on pain monitoring paradigm for tendinopathy are: Silbernagel, 2001; Silbernagel, 2007).
Strengthening exercises in this phase will likely include some exercises for calf muscles (i.e., gastrocnemius and soleus muscles) and a few of my favorite exercises for these muscles are standing calf raises (straight and bent knee), seated calf raises, and calf raises on a leg press machine (see pictures below):

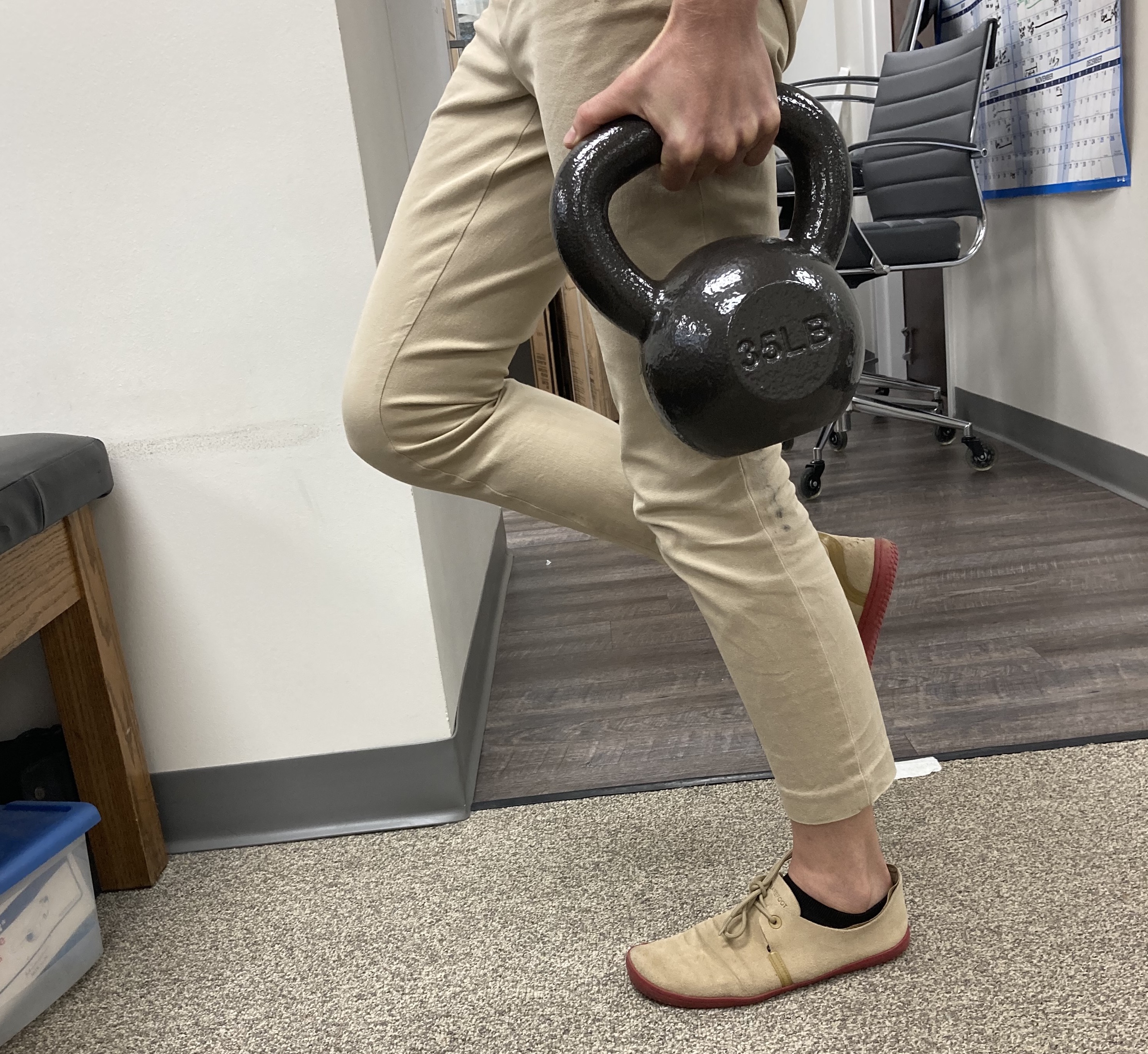



Progression of load is important and often my goal for individuals is to build up to 2-3 days per week of 3-5 sets of heavy single leg calf raises performing 8-12 repetitions in each set. One way to adapt this exercise for those with foot or ankle injuries may be to utilize a “stiff” soled shoe or rigid plate in order to limit toe or foot bending (flexion) but still reap the benefits of the calf strengthening that this exercise can provide. See video below for discussion of this concept:
Footwear Choices for Early Loading in Foot Stress Fractures
Also, it may be advantageous to strengthen muscles that contribute to foot and ankle stability including the posterior tibialis, fibularis muscles, and foot intrinsic muscles. One of my favorite drills for foot arch stability and is the “short foot” exercise or “arch lifts” that can be performed first in sitting, then standing, and finally with dynamic challenges such as a half kneeling press or squat as more challenging variations.
Phase 3: Return to Run
Best prognostic indicators for timelines for return to sport or return to run will be LOCATION and GRADE of bone stress injury (similar to above times for return to weight bearing!).
For a reminder of the official way to determine “Grade” in terms of bone stress injury, I would encourage you to take a look at Part 1: Classifying “Bone Stress Injuries” and Tips for Prevention
Bone Stress Injuries at “Low-Risk” sites that are “Low-Grade” may have the quickest potential of returning to running or sports, with estimates for Grade 1 injuries returning as early as 2-3 weeks (Kijowski, 2012), but most estimates for Grades 1-3 returning around 8 weeks (Dobrindt, 2012; Kahanov, 2015). BSIs at “High-Risk” sites and/or “High-Grades” of injury may take up to 20 weeks to return to sport (Dobrindt, 2012; Kahanov, 2015), with some estimates as long as 32 weeks for stress fractures (Grade 4 injuries) (Nattiv, 2013)!
However, timelines are highly variable and progression will depend on healing of the injury likely assessed via follow up MRIs and also clinical presentation including leg strength, presence or absence of pain with exercise or walk/jog progressions, and other recovery parameters discussed above such as sleep, stress, and nutrition.
It is important to progress slowly with return to running to allow for adaptive changes of the bone and reduce the risk of reinjury or poor healing. Factors that may guide return to running volume will include the individual’s pre-injury fitness and running volume. It is generally recommended that early return to run training include slower speed running bouts and allow for recovery days in between running bouts to assess tolerance to the introduction of this higher demand activity.
For a summary of rehabilitation activities and goals through these different phases, see the chart below:
| PHASE 1 REHAB Activity Modification | PHASE 2 REHAB Strengthening & Walk/Jog | PHASE 3 REHAB: Return to Run |
| Activities (Adapt Loading): Stop running Cross train for conditioning Initiate leg strength exercises Pain guides activity crutches/boot/brace to offload | Activities (Walk/Jog Program): Begin once walking is pain free (1-2 weeks in a row) Initiate Anti-gravity treadmill jogging (start 50% body weight) Progress Anti-G treadmill jogging (by 5-10% body weight per week) | Activities (Return to Run): Begin slow running at low volume (30-50% of pre-injury volume) Progress running distance (about 10% per week) Build strength before speed Gradually introduce plyometrics |
| Goals: Pain free ADLs Maintain aerobic fitness Optimize recovery factors (sleep, nutrition, stress) | Goals: Pain free exercise and walk/jog Gradual increase in walk/jog Maintain/increase leg strength | Goals: Pain free with running Gradual increase in running volume Progress volume/distance before speed! |
References:
- Bennell, KL, Malcolm, SA, Thomas, SA, Wark, JD, & Brukner, PD. The Incidence and Distribution of Stress Fractures in Competitive Track and Field Athletes: A Twelve-Month Prospective Study. The American Journal of Sports Medicine. 1996; 24(2), 211–217.
- Current Concepts of Orthopaedic Physical Therapy 4th Ed. Orthopaedic Section, APTA, Inc.; 2016.
- Dobrindt O, Hoffmeyer B, Ruf J, et al. Estimation of return-to-sports-time for athletes with stress fracture – an approach combining risk level of fracture site with severity based on imaging. BMC Musculoskelet Disord. 2012;13(1):139.
- Fredericson M, Bergman AG, Hoffman KL, Dillingham MS. Tibial Stress Reaction in Runners: Correlation of Clinical Symptoms and Scintigraphy with a New Magnetic Resonance Imaging Grading System. Am J Sports Med. 1995;23(4):472-481.
- Galbraith RM, Lavallee ME. Medial tibial stress syndrome: conservative treatment options. Curr Rev Musculoskelet Med. 2009;2(3):127-133.
- Kahanov L, Eberman L, Games K, Wasik M. Diagnosis, treatment, and rehabilitation of stress fractures in the lower extremity in runners. Open Access J Sports Med. 2015; 6:87-95.
- Kijowski R, Choi J, Shinki K, Del Rio AM, De Smet A/ Validation of MRI classification system for tibial stress injuries. AJR Am J Roentgenol. 2012; 198(4):878–884.
- Kinoshita K, Okada K, Saito I, et al. Alignment of the rearfoot and foot pressure patterns of individuals with medial tibial stress syndrome: A cross-sectional study. Physical Therapy in Sport. 2019;38:132-138.
- Liem BC, Truswell HJ, Harrast MA. Rehabilitation and Return to Running After Lower Limb Stress Fractures: Current Sports Medicine Reports. 2013;12(3):200-207.
- Matcuk GR, Mahanty SR, Skalski MR, Patel DB, White EA, Gottsegen CJ. Stress fractures: pathophysiology, clinical presentation, imaging features, and treatment options. Emerg Radiol. 2016;23(4):365-375.
- Nattiv A, Kennedy G, Barrack MT, et al. Correlation of MRI Grading of Bone Stress Injuries With Clinical Risk Factors and Return to Play: A 5-Year Prospective Study in Collegiate Track and Field Athletes. Am J Sports Med. 2013;41(8):1930-1941.
- Patel DS. Stress Fractures: Diagnosis, Treatment, and Prevention. 2011;83(1):8.
- Reinking MF, Austin TM, Richter RR, Krieger MM. Medial Tibial Stress Syndrome in Active Individuals: A Systematic Review and Meta-analysis of Risk Factors. Sports Health. 2017;9(3):252-261.
- Shaffer SW, Uhl TL. Preventing and treating lower extremity stress reactions and fractures in adults. J Athl Train. 2006;41(4):466-469.
- Silbernagel KG, Thomeé R, Eriksson BI, Karlsson J. Continued sports activity, using a pain-monitoring model, during rehabilitation in patients with Achilles tendinopathy: A randomized controlled study. The American Journal of Sports Medicine. 2007; 35(6):897-906.
- Silbernagel KG, Thomeé R, Thomeé P, Karlsson J. Eccentric overload training for patients with chronic Achilles tendon pain—a randomized controlled study with reliability testing of the evaluation methods. Scand J Med Sci Sports. 2001; 11:197-206.
- Tenforde AS, Kraus E, Fredericson M. Bone Stress Injuries in Runners. Physical Medicine and Rehabilitation Clinics of North America. 2016;27(1):139-149.
- Warden SJ, Davis IS, Fredericson M. Management and Prevention of Bone Stress Injuries in Long-Distance Runners. J Orthop Sports Phys Ther. 2014;44(10):749-765.

2 Comments Add yours