I have been hearing more and more people referring to lateral hip pain with the diagnostic label of “Greater Trochanteric Pain Syndrome” (GTPS). This got me curious about when this was first described as a “syndrome” and what the diagnosis of GTPS is all about. I am not sure who first used this label, but the earliest reference article that I could find with the term “Greater Trochanteric Pain Syndrome” was from 199613.
As I’ve written about before (“Are Labels Helpful or Hurtful in Medicine?”) , we want to make sure that the process of assigning a diagnosis serves a productive purpose and doesn’t just lead to giving someone a negative label to hang onto (something that could arguably contribute to a nocebo or “harming” effect for our patients).
So, what is “Greater Trochanteric Pain Syndrome”? Let’s break it down…
“Greater Trochanteric Pain Syndrome” (GTPS) is lateral hip pain or pain around the greater trochanter that tends to present with a consistent set of signs and symptoms. Remember that a syndrome is just a constellation of signs and symptoms that tend to occur together in a health condition or pathology8 . Common GTPS signs, symptoms, and related pathology are3,4,10 :
- Pain at/near the greater trochanter
- Pain aggravated by activity (walking, running)
- Pain aggravated by certain positions (prolonged standing/sitting, lying on one’s side)
- Pain radiating to the thigh or buttock
- Gluteus medius tendinopathy*
- Trochanteric or hip bursitis**
- IT band tightness/pain
*Gluteal tendinopathy is a more common cause for lateral hip pain vs. bursa** as originally thought (see below for discussion).
A shift in terminology to describe lateral hip pain localized near the greater trochanter has taken place. Whereas it used to be designated most commonly as “trochanteric bursitis”, now the term “Greater Trochanteric Pain Syndrome” is used because of the findings that involvement of the bursa is less common and likely as a pain generator than regional structures such as gluteal tendons and muscles, IT band, and fascia 1,3,4,10,13 .
GTPS tends to occur more often in females than males (from 2 to 4x more often) and is most common in 40-60 year old age groups and those with higher Body Mass Index (BMI)3,10 . It can occur in athletes or sedentary populations, runners, walkers etc.; and the “mechanism of injury” tends to be one of repetitive overuse where there is an increase in loading at the lateral hip. Thus, it is commonly related muscle/tendon pathology (primarily gluteus medius, but also could be gluteus minimus or tensor fascia lata) as those structures are sensitive to excess compression and/or tensile loads. Tendinopathic stages have been described as a “continuum model” of acute irritation using terms such as: “Reactive” vs. “Reactive on Degenerative”2 . They have also been described in terms of duration of symptoms: acute (<4 weeks), subacute (5-12 weeks), chronic (> 12 weeks) or “acute on chronic”11 .
A thorough evaluation is important with patients who present with lateral hip pain; not only to rule in/out the proper diagnosis and stage patient irritability, but also to assess for other comorbidities. Even though GTPS is a broad diagnosis in that it encompasses a “syndrome” (again: group of signs/symptoms), it is important to note that GTPS can co-occur with other regional pathologies. Factors such as low back pain and knee osteoarthritis (OA) have been associated with GTPS12and by one estimate up to2/3 of those with GTPS can have concurrent LBP or hip OA10.
A few tips on evaluating patients with GTPS:
- SCREEN THE LUMBAR SPINE and regional structures for potential pain referrals (gluteus medius, TFL, IT band etc.)
- LOWER EXTREMITY KINETIC CHAIN ASSESSMENT: check for presence of symptoms suggestive of OA (i.e., hip and knee), also assess the foot and ankle
- RULE IN/OUT TENDINOPATHY: (see HEREfor more thorough discussion of common characteristics of lower extremity tendinopathy and assessment)
- LOAD TEST WITH SPECIFIC TESTS for gluteus medius muscle/tendon*(as indicated based on likely involvement of gluteus medius tendinopathy)
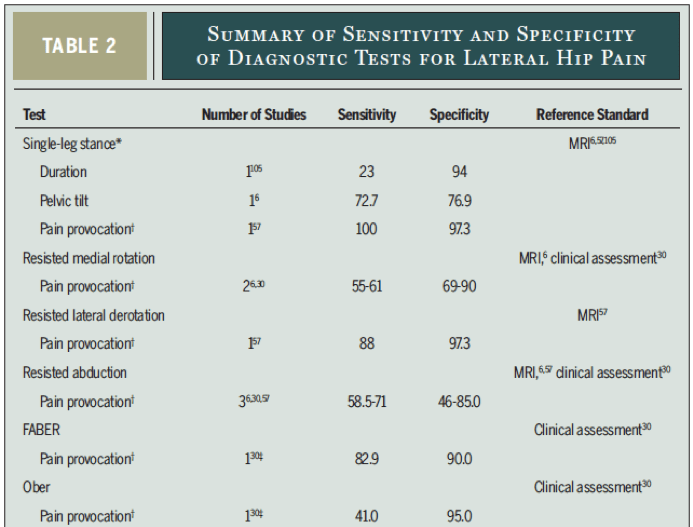
- Resisted External Rotation test (aka “resisted lateral derotation”) (good sensitivity and specificity)
- FABER Test (good sensitivity and specificity)
- Ober’s Test (good specificity, POOR sensitivity, so good test to rule IN diagnosis if the test is POSITIVE!)
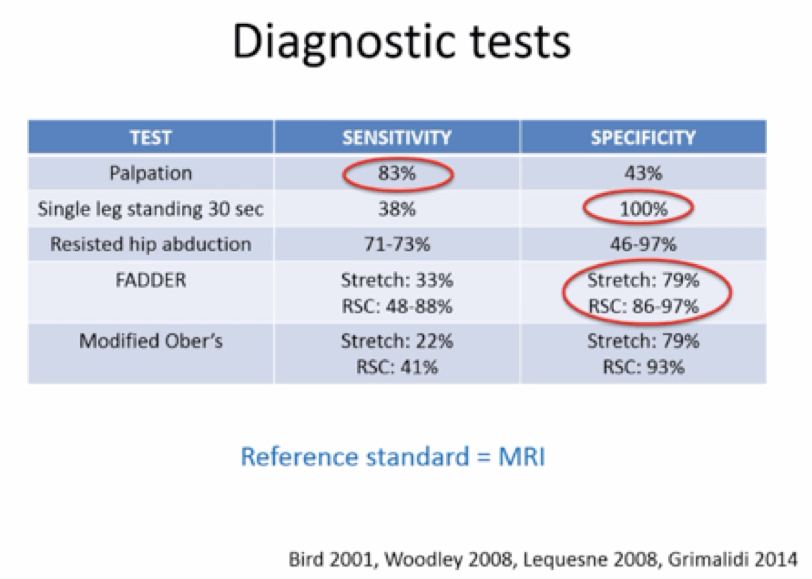
- Palpation (at greater trochanter) good sensitivity, POOR specificity, so good test to rule OUT diagnosis if the test is NEGATIVE!)
*See “Table 2” below from Grimaldi & Fearon, 20154 for sensitivity and specificity of these tests:
Also “Diagnostic tests” table: from physiotherapist Dr. Peter Malliaras’ course on Treatment of Lower extremity tendinopathies7, the figure below refers to Gluteal Tendinopathy Diagnostic tests:
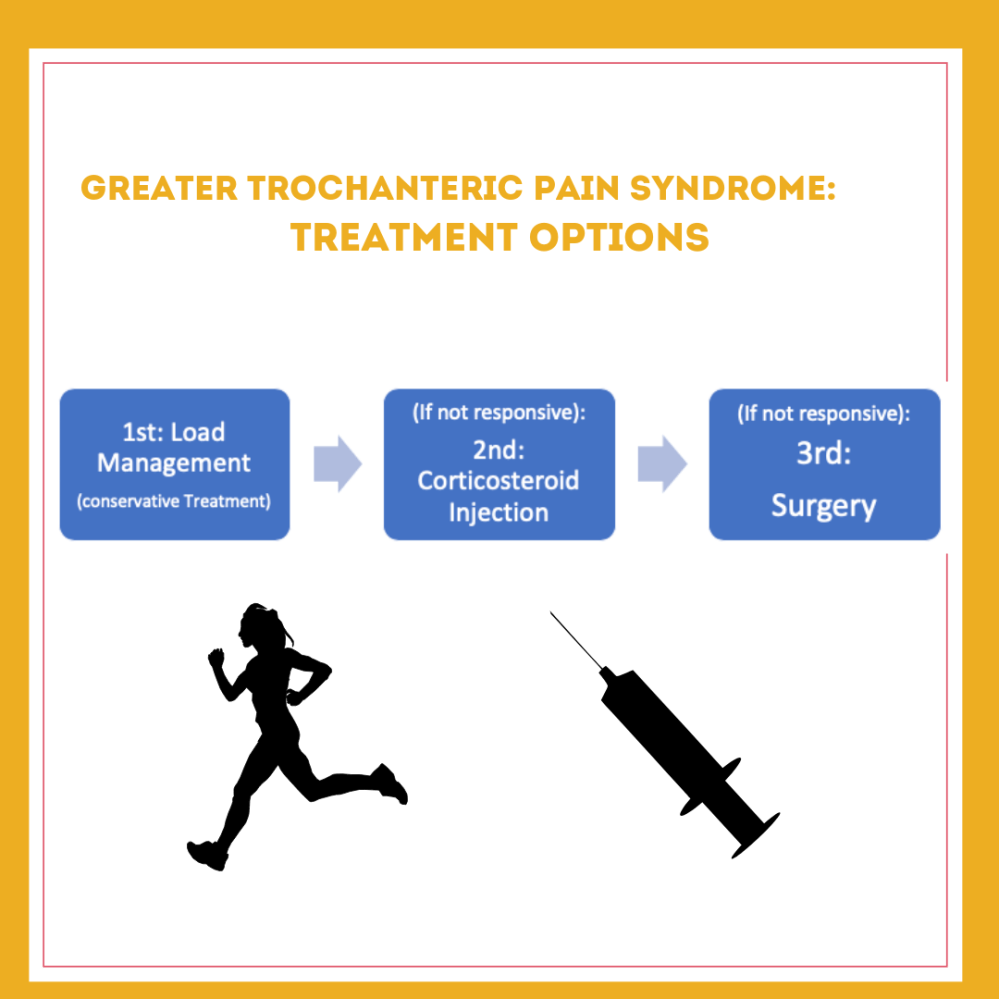
How do we TREAT GTPS?????
The keys to treating GTPS are similar to how you would go about treating a gluteal tendinopathy* due to the likely presence of this pathology within the “Syndrome” of GTPS. Treating GTPS should include:
- Patient Education
- Activity Modification/Avoid Aggravating Positions
- Therapeutic Loading/Exercises
*For a more in-depth discussion of managing tendinopathies please see my series on assessment and treatment of lower extremity tendinopathies as well as case studies.
- PATIENT EDUCATION (should include information on diagnosis, treatments, prognosis):
PATIENT EDUCATION ON DIAGNOSIS OF GTPS: discuss signs and symptoms as listed above that are related to GTPS and associated risk factors/co-morbiditis if present (sex, age, presence of low back pain or OA).
PATIENT EDUCATION ON TREATMENT OPTIONS (PROS/CONS):
A good way to think about treatment decisions, is to look at effectiveness of treatment as well as possible risks (e.g., “Cost-Benefit” analysis). A brief assessment of common treatments for GTPS reveals the following:
| TREATMENT OPTIONS | RISK/COST | BENEFITS
(short term vs. long term) |
| PATIENT EDUCATION + EXERCISE
(Load Management)
|
LOW | Short term (0-4 wks): LOW benefit
Long Term: HIGH benefit |
| CORTICOSTEROID INJECTIONS
(or Dry Needling, see below for comparison)
|
MEDIUM |
Short Term (0-4 wks): HIGH benefit
Long Term: LOW/NO benefit |
|
SURGERY |
HIGH
|
Long Term: HIGH benefit |
Studies on EXERCISE interventions reveal:
- EDUCATION PLUS EXERCISE has better long-term pain/function improvements vs. corticosteroid injections and “wait and see” approach for glute tendinopathy8
(Figure below from Mellor et al., 2018)8:
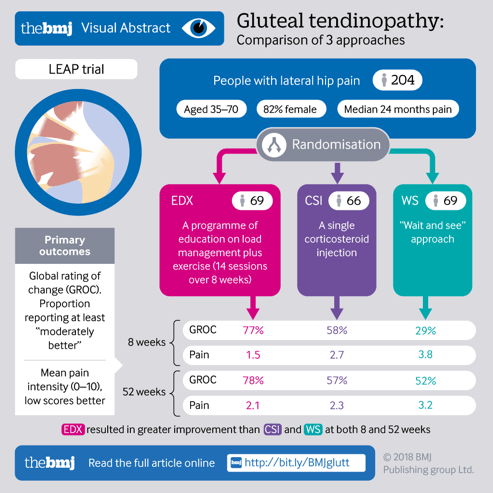
- EXERCISE HAS GOOD LONG-TERM BENEFITS (BUT MAY NOT SHOW SHORT-TERM IMPROVEMENTS), In one study on patients with gluteal tendinopathy receiving an exercise treatment intervention4:
- 7% of patients reported improvement at 4 weeks
- 40% of patients reported improvement at 4 months
- 80% of patients reported improvement at 15 months
Studies on OTHER TREATMENT options reveal:
Dry Needling and Corticosteroid Injections:
- Dry Needlingperformed just as well as corticosteroid injections for improvements in pain, function, and reduced medication intake in treating GTPS as measured after 1, 3, 6 weeks1
- *Plus dry needling may carry less risk vs. injections
- Corticosteroid Injections:may provide some short-term pain relief(for 4 weeks) but long-term outcomes are not as good as exercise/education-based interventions (pain relief at 12 months after injection)!
- Review of studies: reported that corticosteroid injections reduced pain at 4 weeks for about 75% of patients, but at 3-4 months was only 40-50% and at 12 months there was no difference in pain between the injections and regular analgesics as needed!4
- Injections= strong evidence for ST relief
Shock Wave Therapy (Extracorporeal Shockwave Therapy (ESWT):
- some research support, could try it if you have access to it10
Surgery:6,10
- Surgery could involve IT band or TFL/gluteal tendon resection or repair, bursectomy, or osteotomy of greater trochanter
- Surgery is effective in recalcitrant cases: good patient reports post-surgery for improved pain and function, but
- Surgery is usually not recommended until conservative treatment fails
PATIENT EDUCATION ON PROGNOSIS:
- Most patients respond to conservative treatment(e.g., patient education, exercise interventions, load management)6
- Tendinopathy may take longer to recoverdue to its “overuse” mechanism of injury as well as the proposed structural and neuromodulatory mechanisms proposed for recovery7
*Importance of Patient Education: In one study that looked at effects of exercise, even though the exercise group responded well, there were no differences in muscle strength between groups and authors suggest that some of the utility of the “exercise” intervention was in the form of patient education to avoid provoking positions and also load management.8
2. ACTIVITY MODIFICATION/AVOID AGGRAVATING POSITIONS:
- Activity Modification:
- Walk with a walking pole/stick to offload hip abductors (glute med/min),
- Use a “pain monitoring model” to keep pain < 3/10 and adjust activity accordingly
- Avoid Aggravating Positions:
- In the short term: no stretching of lateral structures (IT band, hip abductor muscles)
- Avoid crossing legs in sitting
- If sleeping in side lying position: place a pillow between the legs/knees
- No stretching of the leg across the body
- Can use a cushion in sitting to improve comfort
3. THERAPEUTIC LOADING/EXERCISES
-
- Important to load with in a “therapeutic range” (see specifics HERE).
- Too little load is bad, too much load is bad
- We want to optimize remodeling of these tissues (muscle, connective tissue, etc.)5
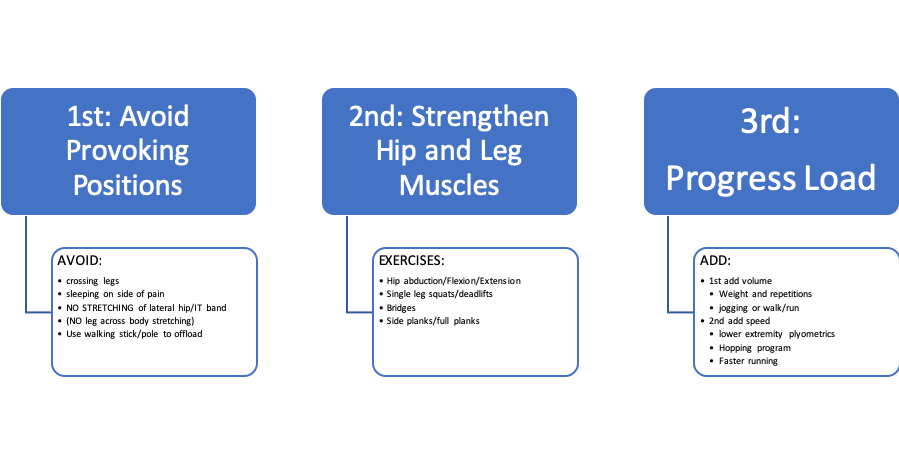
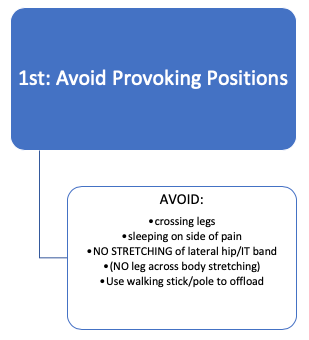
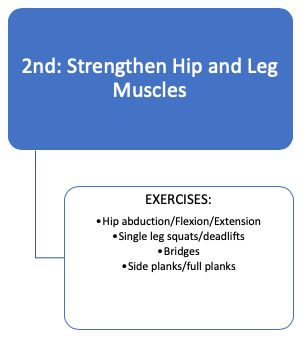
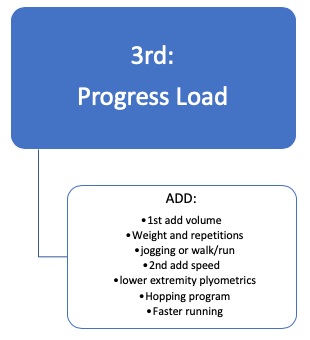
THERAPEUTIC LOADING THROUGH STAGES OF TREATMENT:
References (GTPS):
- Brennan KL, Allen BC, Maldonado YM. Dry Needling Versus Cortisone Injection in the Treatment of Greater Trochanteric Pain Syndrome: A Noninferiority Randomized Clinical Trial. J Orthop Sports Phys Ther. 2017;47(4):232-239.
- Cook JL, Rio E, Purdam CR, Docking SI. Revisiting the continuum model of tendon pathology: What is its merit in clinical practice and research? British Journal of Sports Medicine. 2016;50(19):1187-1191.
- Del Buono A, Papalia R, Khanduja V, Denaro V, Maffulli N. Management of the greater trochanteric pain syndrome: a systematic review. British Medical Bulletin. 2012;102(1):115-131.
- Grimaldi A, Fearon A. Gluteal Tendinopathy: Integrating Pathomechanics and Clinical Features in Its Management. J Orthop Sports Phys Ther. 2015;45(11):910-922.
- Hart DA, Scott A. Getting the dose right when prescribing exercise for connective tissue conditions: The Yin and the Yang of tissue homeostasis. Br J Sports Med. 2012;46(10):696-698.
- Lustenberger DP, Ng VY, Best TM, Ellis TJ. Efficacy of Treatment of Trochanteric Bursitis: A Systematic Review: Clinical Journal of Sport Medicine. 2011;21(5):447-453.
- Malliaras P. Mastering Lower Limb Tendinopathy 2nd https://www.tendinopathyrehab.com/Accessed: December 18th, 2018.
- Mellor R, Bennell K, Grimaldi A, et al. Education plus exercise versus corticosteroid injection use versus a wait and see approach on global outcome and pain from gluteal tendinopathy: prospective, single blinded, randomised clinical trial. The British Medical Journal. 2018; 361:k1662.
- https://www.merriam-webster.com/dictionary/syndrome
- Reid D. The management of greater trochanteric pain syndrome: A systematic literature review. Journal of Orthopaedics. 2016;13(1):15-28.
- Scott A, Backman LJ, Speed C. Tendinopathy: Update on Pathophysiology. J Orthop Sports Phys Ther. 2015;45(11):833-841.
- Segal NA, Felson DT, Torner JC, et al. Greater Trochanteric Pain Syndrome: Epidemiology and Associated Factors. Archives of Physical Medicine and Rehabilitation. 2007;88(8):988-992.
- Shbeeb MI, Matteson EL. Trochanteric bursitis (greater trochanter pain syndrome). Mayo Clin Proc 1996;71:565–569.

4 Comments Add yours