In our Western culture and media, we are very focused on image and outward appearance. Even in the wellness industry that claims to promote health, there is a stereotyped image and the implicit message that obtaining this look is what it means to be “healthy” (i.e., low body fat, blemish-free skin, muscle definition etc.). However, this perpetuation of a certain “ideal look” can have detrimental effects. For example, a well-known study, conducted in the 1990s investigated the negative influence that the introduction of Western television had on girls’ body image2,3. Sadly, body image dissatisfaction and disordered eating drastically increasedafter the introduction of Western media and these behaviors seemed to correspond with the girls’ reports of a desire to look like and emulate the characters they saw on television.
Exposure to these media images was harmful and much has been written since about the detrimental effects that media can have on body image and eating behaviors (e.g., Spetigue & Henderson, 2004)21. We may be seeing a similar crisis with the utilization and hyper-focus on diagnostic imaging within Western medicine (e.g., x-rays, Magnetic Resonance Imaging (MRI), Computerized Axial Tomography (CAT or CT scans)).
What if exposure to diagnostic imaging (e.g., X-rays, MRIs) was equally as damaging to our “body images” and how people feel about their worth and ability?
What we are beginning to understand is that this is not far from the truth. An overreliance on ordering imaging for musculoskeletal disorders and how we talk about imaging findingswith our patients could be harming them instead of enhancing our diagnosis and treatment4,7,22,24.
Another useful analogy taken from research on body image is that of the undue focus on body weight or body mass index (BMI) as indicators of health. Though these two measurements can be useful as parts of a broad examination of health, they are in no way a completepicture of the health of an individual. Likewise, an x-ray or MRI is just one piece of information that must be interpreted in the greater context of a comprehensive clinical exam (made up of many factors!). As a reminder, this exam should focus MOST SIGNIFICANTLY on FUNCTION!
During my time working in research and prevention of eating disorders, part of our mission was to shift the focus from the culturally reinforced “Thin-Ideal Look” to a more appropriate “Healthy-Ideal” that emphasizes engaging in behaviors that promote physical health, mental health, and quality of life. The time is ripe for a similar paradigm shift in medicine and also in physical therapy to prioritize FUNCTION and BEHAVIORS not an image!
The first step in this paradigm shift is to acknowledge the shortcomings of diagnostic imaging (X-rays, MRIs) and the ways in which images can harm instead of help. With that direction in mind, here are two points that I think are worth making:
- IMAGING FINDINGS DO NOT AUTOMATICALLY MEAN SOMETHING NEEDS “FIXED”!
- OVERRELIANCE ON IMAGING CAN BE HARMFULAND COSTLY!
IMAGING FINDINGS DO NOT
AUTOMATICALLY MEAN SOMETHING NEEDS “FIXED”!
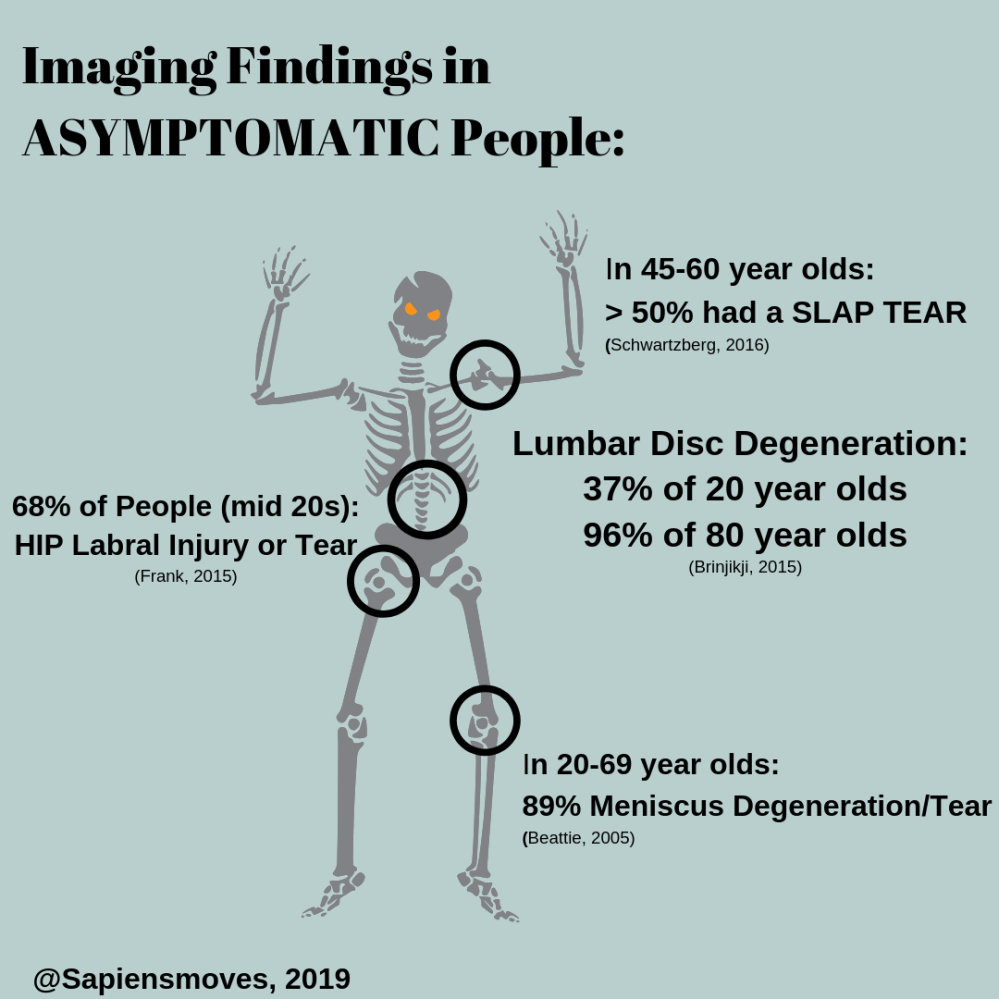
So-called “pathological” findings on imaging studies do not mean something needs “fixed”. There are many examples of populations of individuals who are asymptomatic (read: functioning just fine!) that have “pathological” findings on imaging studies. See below for some of these examples (by body region):
LUMBAR SPINE IMAGING:
- 36% of asymptomatic people had CAT scans that were interpreted as having “Significant Lumbar Abnormality” (e.g., disc bulge, stenosis, facet degeneration) (Wiesel, 1984)25
- “Disc Degeneration” in lumbar spine CT or MRI scans in ASYMPTOMATIC individuals was found in 37% of 20 year olds! (and increased to 96% of 80 year olds!) (From a systematic review of 33 studies) (Brinjikji et al., 2015)5
CERVICAL SPINE IMAGING:
- Out of 1,211 healthy people (ages 20-70 years old and asymptomatic): (Nakashima, 2015)16
- 86% had “Disc Bulges” on their Cervical Spine MRI scans
- about 75% of those in their 20s had “Disc Bulges”
TEMPOROMANDIBULAR JOINT (TMJ) IMAGING:
- 9% to 31% of asymptomatic people have (TMJ) disc displacements on MRI scans (De Leeuw, 2013)6
- No correlation was found between clinical markers of TMJ dysfunction (local pain/tenderness) and radiographic changes in a sample of 39 with TMJ dysfunction(Nordahl, 1997)17
SHOULDER IMAGING:
- In a sample of 53 ASYMPTOMATIC middle-aged individuals (male, female ages 45-60 years old), MRI scans showed: (Schwartzberg, 2016)20
- OVER HALF WERE DIAGNOSED with SUPERIOR LABRAL TEARS (“SLAP” Injuries) (55% or 72% depending on the radiologist reading the MRI)
- In a sample of 51 healthy males (40-70 years old) with NO SHOULDER SYMPTOMS (upon Ultrasound exam): (Girish, 2011)10
- 78% had bursal (sub acromial or deltoid) thickening
- 66% had acromioclavicular joint osteoarthritis
- 22% had a PARTIAL ROTATOR CUFF TEAR (supraspinatus)
- In a sample of 664 individuals (male and female, 20-87 years old) (upon Ultrasound exam) (Minagawa, 2013)15
- 22% had FULL THICKNESS ROTATOR CUFF TEAR (Increasing prevalence with increasing age) – out of those with tears: 65% were ASYMPTOMATIC (2x as many asymptomatic tears as symptomatic tears)!
HIP IMAGING:
- In a systematic review (26 studies, 2,114 people, male and female, average age: 25.3 +/- 1.5 years old) of CT or MRI scan findings in ASYMPTOMATIC individuals: (Frank, 2015)8
- 68% had a HIP LABRAL INJURY or TEAR
- 67% had a “PINCER DEFORMITY” suggestive of bony morphological change common in femoral acetabular impingement (FAI)
- 37% had a “CAM DEFORMITY” suggestive of bony morphological change common in femoral acetabular impingement (FAI)
- In a sample of 45 healthy ASYMPTOMATIC individuals (male and female, age 15-66 years old), MRI scans revealed (Register, 2012)19
- Abnormalities in 73% of hips, including:
- 69% with LABRAL TEARS!
- 24% with chondral defects
- 11% acetabular rim fractures
- Abnormalities in 73% of hips, including:
KNEE IMAGING:
- Using data from the “Framingham OA Study”, out of 710 Individuals (male and female, > 50 years old) WITHOUT Knee OA(Guermazi, 2012)11
- 87% of those WITHOUT PAIN IN THEIR KNEEShad ABNORMALITIES ON KNEE MRIs (e.g. osteophytes, cartilage defects, etc.)
- In a sample of ASYMPTOMATIC individuals (20-69 years old) (Beattie, 2005)1
- 89% had a MENISCUS ABNORMALITY (degeneration or tear) (located at the posterior horn of medial meniscus) on MRI
- 27% had OSTEOPHYTES (bone spurs) at their knee (tibia, femur, or patella) on X-Ray or MRI
ANKLE IMAGING:
- In a sample of 48 ASYMPTOMATIC individuals, Ultrasound exam of the foot showed (Symeonidis, 2012)23
- 54% had “Neuromas” (nerve thickening) between their toes (i.e., Morton’s Neuromas)
- In a sample of 320 individuals (male, female, median age: 51 years old) who were ASYMPTOMATIC and with NO HISTORY OF ANKLE TRAUMA OR INSTABILITY, MRI scans showed (O’Neil, 2017)18
- 37% HAD ABNORMALITY OF ATFL (anterior talofibular ligament, thickening, tear, degeneration)
Also, just because your imaging findings come back “negative” does not mean nothing is wrong. The image is only as good as our technology that represents this “look” inside the body and there are human beings interpreting these images, and human beings make mistakes. Evidence of this concept is that radiologists may miss fractures (i.e., broken bones) or other musculoskeletal pathology such as dislocations that could be diagnosed via imaging techniques such as x-rays or MRIs12,13.
OVERRELIANCE ON IMAGING CAN BE HARMFUL AND COSTLY!
Our best current evidence for management of non-specific low back pain suggests that imaging should NOT be ordered unless red flag symptoms are present (e.g., progressive neurologic deficits), serious underlying pathology is suspected (e.g. cancer or fracture), or a patient is a surgical candidate or not responding to conservative care7, 14. Furthermore, research suggests that many cases of non-specific low back pain do NOT have a pathoanatomical cause and the overwhelming majority of individuals with low back pain do NOT require diagnostic imaging7, 24. Despite these recommendations and evidence, diagnostic imaging for low back pain continues to be over utilized and may be recommended or obtained in OVER 50% of inappropriate cases7, 24.

This over reliance and inappropriate use of imaging cannot be taken lightly as it affects not only our health care costs as a society, but can actually be harmful to patients’ physical and psychological health! In fact, some patients with “pathological” imaging findings of their spines, yet NO SYMPTOMS have undergone surgery seemingly due to the imaging findings alone!24 . Research has demonstrated that risks associated with overusing imaging include exposure to radiation, overutilization of surgical techniques and diagnostic “labelling” with pathoanatomic diagnoses that may be inaccurate at best and pathologize what may be best described as normal, age-related changes7. Physical therapists have a key role to play in how imaging is viewed and used by patients. A recent study conducted on patients with low back pain, found that those that saw a physical therapist first were less likely to obtain expensive imaging studies9.
As these findings suggest, we must be diligent with our conversations regarding the benefits or risks of pursuing imaging studies as well as the limitations of imaging. We must be especially cautious in order to avoid creating iatrogenic or nocebo effects with our patients (i.e., the medical adage of “primum non nocere” or “First, do no harm”)4, 22.
With this in mind, a simple reminder may be in order to our patients:
YOU ARE NOT YOUR X-RAY
Free Info Graphic Download (Asymptomatic Findings on Imaging)
References:
- Beattie KA, Boulos P, Pui M, et al. Abnormalities identified in the knees of asymptomatic volunteers using peripheral magnetic resonance imaging. Osteoarthritis and Cartilage. 2005;13(3):181-186.
- Becker AE. Television, Disordered Eating, and Young Women in Fiji: Negotiating Body Image and Identity during Rapid Social Change. Cult Med Psychiatry. 2004;28(4):533-559.
- Becker AE, Burwell RA, Herzog DB, Hamburg P, Gilman SE. Eating behaviours and attitudes following prolonged exposure to television among ethnic Fijian adolescent girls. Br J Psychiatry. 2002;180(06):509-514.
- Bedell SE, Graboys TB, Bedell E, Lown B. Words That Harm, Words That Heal. Archives of Internal Medicine. 2004;164 (13): 1365-8.
- Brinjikji W, Luetmer PH, Comstock B, et al. Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. AJNR Am J Neuroradiol. 2015;36(4):811-816.
- De Leeuw R, Klasser GD, eds. Orofacial Pain: Guidelines for Assessment, Diagnosis, and Management. 5th Hanover Park, IL. Quintessence Publishing; 2013.
- Flynn TW, Smith B, Chou R. Appropriate Use of Diagnostic Imaging in Low Back Pain: A Reminder That Unnecessary Imaging May Do as Much Harm as Good. Journal of Orthopaedic & Sports Physical Therapy. 2011;41(11):838-846.
- Frank JM, Harris JD, Erickson BJ, et al. Prevalence of Femoroacetabular Impingement Imaging Findings in Asymptomatic Volunteers: A Systematic Review. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2015;31(6):1199-1204.
- Frogner BK, Harwood K, Andrilla CHA, Schwartz M, Pines JM. Physical Therapy as the First Point of Care to Treat Low Back Pain: An Instrumental Variables Approach to Estimate Impact on Opioid Prescription, Health Care Utilization, and Costs. Health Services Research. May 2018.
- Girish G, Lobo LG, Jacobson JA, Morag Y, Miller B, Jamadar DA. Ultrasound of the Shoulder: Asymptomatic Findings in Men. American Journal of Roentgenology. 2011;197(4):W713-W719.
- Guermazi A, Niu J, Hayashi D, et al. Prevalence of abnormalities in knees detected by MRI in adults without knee osteoarthritis: Population based observational study (Framingham Osteoarthritis Study). BMJ. 2012;345(aug29 1):e5339-e5339.
- Gyftopoulos S, Chitkara M, Bencardino JT. Misses and Errors in Upper Extremity Trauma Radiographs. American Journal of Roentgenology. 2014;203(3):477-491.
- Ha AS, Porrino JA, Chew FS. Radiographic Pitfalls in Lower Extremity Trauma. American Journal of Roentgenology. 2014;203(3):492-500.
- Lin I, Wiles L, Waller R, et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. Br J Sports Med. March 2019:bjsports-2018-099878.
- Minagawa H, Yamamoto N, Abe H, et al. Prevalence of symptomatic and asymptomatic rotator cuff tears in the general population: From mass-screening in one village. Journal of Orthopaedics. 2013;10(1):8-12.
- Nakashima H, Yukawa Y, Suda K, Yamagata M, Ueta T, Kato F. Abnormal Findings on Magnetic Resonance Images of the Cervical Spines in 1211 Asymptomatic Subjects: Spine. 2015;40(6):392-398.
- Nordahl S, Alstergren P, Appelgren A, Appelgren B, Eliasson S, Kopp S. Pain, tenderness, mandibular mobility, and anterior open bite in relation to radiographic erosions in temporomandibular joint disease. Acta Odontol Scand. 1997;55:18–22.
- O’Neil J, McDonald E, Chapman T, Casper D, Shakked R, Pedowitz D. Anterior Talofibular Ligament Abnormalities on Routine Magnetic Resonance Imaging of the Ankle. Foot & Ankle Orthopaedics. 2017;2(3):2473011417S0003.
- Register B, Pennock AT, Ho CP, Strickland CD, Lawand A, Philippon MJ. Prevalence of Abnormal Hip Findings in Asymptomatic Participants: A Prospective, Blinded Study. Am J Sports Med. 2012;40(12):2720-2724.
- Schwartzberg R, Reuss BL, Burkhart BG, Butterfield M, Wu JY, McLean KW. High Prevalence of Superior Labral Tears Diagnosed by MRI in Middle-Aged Patients With Asymptomatic Shoulders. Orthopaedic Journal of Sports Medicine. 2016;4(1).
- Spettigue W, Henderson KA. Eating disorders and the role of the media.Can Child Adolesc Psychiatr Rev. 2004 Feb;13(1):16–9.
- Stewart M, Loftus S. Sticks and Stones: The Impact of Language in Musculoskeletal Rehabilitation. Journal of Orthopaedic & Sports Physical Therapy. 2018;48(7):519-522.
- Symeonidis et al. (2012) foot and ankle “Prevalence of Interdigital Nerve Enlargements in an Asymptomatic Population”
- Tousignant-Laflamme Y, Longtin C, Brismée J-M. How radiological findings can help or hinder patients’ recovery in the rehabilitation management of patients with low back pain: what can clinicians do? Journal of Manual & Manipulative Therapy. 2017;25(2):63-65.
- Wiesel SW, Tsourmas N, Feffer HL, Citrin CM, Patronas N. A Study of Computer-Assisted Tomography: I. The Incidence of Positive CAT Scans in an Asymptomatic Group of Patients. 1984; 9(6).

4 Comments Add yours