How many people do you know who have had low back pain at some point in their life?
My guess would be A LOT!
Low back pain is incredibly common and is the leading cause of disability world-wide (Hartvigsen, 2018).
Because it is so ubiquitous, low back pain has been referred to as an “epidemic” and has even been equated to the common cold (Buchbinder, 2018; Delitto, 2012; Current Concepts, 2016). Despite its prevalence, back pain does not have to be that harmful. Most people with acute low back pain will get better in about 6-8 weeks with minimal treatment. (Current Concepts, 2016).
However, in many cases low back pain is either mismanaged or misunderstood and causes a great deal of healthcare spending and burden of disease. But, just like a common cold, the good news is that treatment for acute low back pain (pain less than 3 months in duration) is often effective and these acute episodes tend to resolve in most cases.
Viewing back pain as pretty normal and in most cases not very harmful (like most colds) can be helpful because it tends to deemphasize the fear associated with acute episodes of low back pain and reduce the belief that low back pain automatically requires medical attention. (Buchbinder, 2018).
“Low back pain is a fairly benign part of daily life” -(adapted from: Buchbinder, 2018)

However, something to keep in mind is that chronic low back pain (pain lasting longer than 3 months) is harder to treat and even with people with acute low back pain, recurrent episodes or “flare-ups” are common. (Current Concepts, 2016). But…it is worth repeating the “cold analogy” and saying that getting a minor illness (a cold) is understandably something that may happen repeatedly…and repeatedly we can repeatedly recover!
So, since low back pain is so common and costs our society so much money, shouldn’t we seek to treat those with low back pain with the most current evidence available? Yes, of course!
The problem is that studies show treatment for low back pain is often delivered in a manner that DOES NOT use current evidence-based recommendations or “clinical practice guidelines” (Foster, 2018).
Here are 3 Big “Errors in Clinical Practice” in Treating Low Back Pain:
-
Imaging is OVER utilized (We are OVERLY Focused on “Pathoanatomy”)
-
Invasive & Aggressive Treatments are OVER utilized
-
Active Treatments are UNDER utilized
-
Imaging is OVER utilized (We are OVERLY Focused on “Pathoanatomy”)
Imaging (e.g., X-rays or MRIs) for those with low back pain is discouraged unless there are findings that may suggest more serious or sinister pathology (Current Concepts, 2016; Delitto, 2012). “Routine Imaging” does NOT improve outcomes for low back pain and in fact could be harmful (Karel, 2015). The overuse of imaging may be especially detrimental because it places undue focus on “Pathoanatomical” causes of back pain (i.e., linking the cause of pain to a specific body tissue) which are NOT well supported in research as the definitive cause of most back pain. Despite these recommendations, imaging in low back pain is overutilized which increases healthcare costs and could cause harmful effects for patients’ health such as increasing fear, disability, and even increased rates of unneeded surgical procedures (Foster, 2018; Flynn, 2011; Tousignant-Laflamme, 2017). In fact, increasing rates of spinal surgery have been found in areas with higher rates of MRI usage (Lurie, 2003).
Furthermore, many studies suggest that individuals without pain can often have abnormal imaging findings. For a deeper discussion of imaging findings in asymptomatic populations see here:
You are NOT Your X-Ray Blog Post
As clinicians working with people with low back pain, we need to refocus our efforts and avoid making low back pain primarily a “tissue issue”.
2. Invasive/Aggressive Treatments are overutilized (e.g., Surgery, injections, opioid medications, etc.) (Foster, 2018)
As mentioned above, most low back pain has a favorable prognosis (i.e., expectation of good recovery) with minimal treatment and “conservative care” such as physical therapy. With this in mind, treatments for low back pain that are invasive or that carry higher risks (e.g., oral medications, injections, surgery) should be used judiciously and only after more conservative measures have been attempted (Current Concepts, 2016). Surgery may not be necessary and in many cases may not even be helpful for low back pain. Up to 1/3 of those getting lumbar surgery for low back pain may still have long term pain and disability (Atlas, 2005; Findlay, 1998; Yorimitsu, 2001).
3. Active Treatments are UNDER utilized: (Foster, 2018)
Early return to work and activity is absolutely indicated for most back pain and so is engaging in a variety of types of exercise.
Remember, our spines and backs are designed to undertake a variety of movements and are inherently very robust and strong! Exercises that could be helpful for low back pain could include weightlifting and a variety of aerobic types of exercise (walking, biking, running etc.) among other forms of movement (Foster, 2018; Current Concepts, 2016).
What Does the “Best Available Evidence” Support for Treatments?
First there is a need to screen for “Red Flags” or indicators that something more serious or sinister may be causing a person’s back pain. These causes of low back pain are not common, but it is important that they be recognized early in order to get the best care possible. For a more thorough discussion of medical screening for low back pain, see:

Physical Therapists’ Role in Medical Screening for Low Back Pain
If screening has ruled out more serious causes of low back pain, we move into treatment for what has been termed “Non-specific” Low Back Pain. Treatment decisions are best guided by how bad the pain and symptoms are (symptom “severity”) and how long they take to calm down once they are stirred up (symptom “irritability”). There is also some research evidence that suggests people may respond best if treatment is matched to certain predictive factors about their back pain like how long it has been going on or what movements make their pain better or worse (i.e., assigning “Treatment-Based Classification”). To simplify…
The 3 Stage Process goes like this:
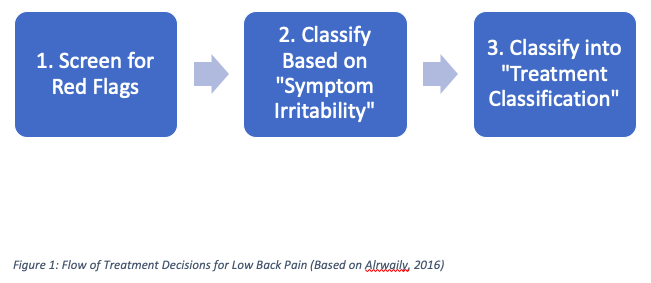
Also, the graphic below may help to understand this 3 Stage approach to evaluation and guiding treatment decisions (Figures Based on: Alrwaily, 2016; DeLitto, 1995; Fritz, 2007).
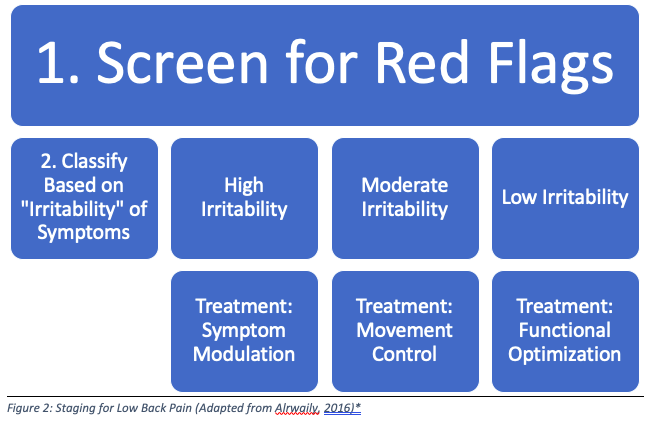
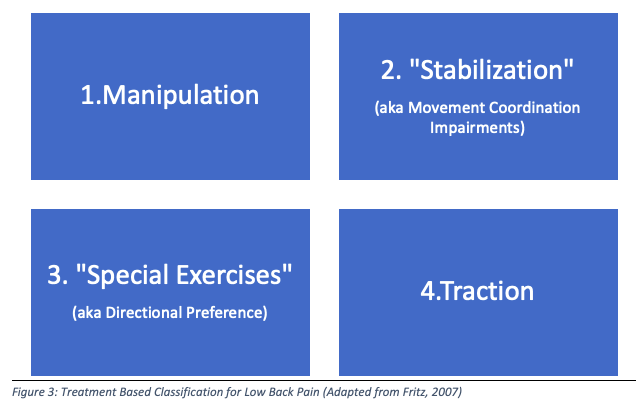
*Stage 3 Includes assigning a “Treatment-Based Classification”, which is described below:
Broadly, evidence suggests that effective treatments will be guided by the foundations of patient education, pain control strategies, and exercise. These should all be a part of a comprehensive treatment program for those with back pain. In most cases, this treatment strategy is effective and prevents the use of more invasive or aggressive treatments like injections or surgery. Physical therapists can help guide these treatments, but ultimately the goal is to empower those with back pain to understand more about possible contributors to pain, engage in regular activity and exercises, and manage “flare-ups” should they occur with adaptive pain control strategies.
Here are 3 “Evidence Based” Treatments to Focus on for Low Back Pain:
(Buchbinder, 2018; Chou, 2017; DeLitto, 2012; Foster, 2018; O’Connell, 2016; O’Connell, 2018; Oliveira, 2018; Qaseem, 2017)
- Patient Education
- Treat Pain
- “Movement is Medicine”
-
Patient Education
Patient education should focus on teaching individuals with back pain research-supported “causes” of back pain, which could include de-emphasizing pathophysiology (“Tissue Issue”), teaching about pain neurobiology, and acknowledging various biopsychosocial contributors to back pain (Louw, 2011; Louw, 2016; Moseley, 2015; Puentedura, 2016). Education should also include discussing the importance of self-management strategies and early return to work and activity including exercise (Buchbinder, 2018; Chou, 2017; Foster, 2018; O’Connell, 2016; O’Connell, 2018; Oliveira, 2018; Qaseem, 2017).
-
Treat Pain
Treating pain with low cost and low risk methods (e.g., physical therapy, low-risk pain medications like over the counter Tylenol or NSAIDs, etc.) could reduce reliance on future invasive treatment options such as surgery or injections (Buchbinder, 2018). Another method for treating pain is to teach patients more about pain neurobiology, often termed “pain neuroscience education” (PNE). It has been shown that PNE can reduce pain and improve function in those with back pain.
-
“Movement is Medicine” = Focus on Exercise-Based Treatments
Exercise and movement is beneficial as part of a healthy lifestyle and for those with back pain, this advice could not be more important! Indeed, “movement is medicine”. But, what exercise or types of exercise are best for low back pain?
There is some support for the idea that certain exercises could be most helpful if they are “matched” to the type of back pain one is experiencing. This aligns with the “Treatment-Based classification” rationale and evidence base (Alrwaily, 2016; DeLitto, 1995; Fritz, 2007). However, it is important to note that there is no “perfect” exercise and the idea that a “weak core” causes back pain is not necessarily true. Also, exercises that aim to train “deep core muscles” like the transverse abdominus and multifid muscles are not necessarily superior to general core exercises targeting larger spinal muscles (Current Concepts, 2016; Fritz, 2007).
My guiding principles for working to improve back pain are to pick exercises based on the goal of the individual and/or the area that most needs to be improved based on broad categories describing overall fitness capacity or movement health:
- Strength and Power
- Mobility and Flexibility
- Movement Variability
- Endurance and Aerobic Fitness
*Note: if nerve sensitivity or irritation is present, I often will use exercises for nerve health. These could include nerve glides or “flossing”, sensory desensitization or sensory discrimination techniques, or even moderate intensity aerobic activity.
Some examples of exercises based on these categories:







Within the category of “Movement variability”, I like to think of those individuals that early on in their back pain tend to feel better moving in a certain direction. In the literature these individuals tend to fall in the “Directional Preference” (aka “special exercises”) category. Initially, exercise selection. May be to LIMIT the direction or variability of their movements, with the ultimate goal of restoring pain free movement in ALL directions and planes of motion.
There are many answers to the question of which exercises are best, but I tend to think that a variety of movement approaches tends to be most helpful. For most patients, the long-term goal would be to increase strength and overall fitness.
Particularly, for those who have had back pain for a while, one of the most effective strategies would be to gradually increase any type of moderate intensity aerobic exercise that does not lead to significant increases in pain. This could be as simple as starting a walking program and performing daily walks of 20-30 minutes or more.
There are many options for beneficial exercise that fall into this category… yoga or circuit training could be great, many types of strength training or weight lifting could be beneficial as could biking, using cardio equipment like an elliptical machine, or even running- as one study showed that runners had increased hydration and bulk of intervertebral discs suggesting that running may be beneficial to “strengthen” the tissues of the spine just like it is for other tissues! (Belavy, 2017).
I hope this post helps to reduce some of the use of overly aggressive treatment options for those with low back pain and put the focus “back” on more effective strategies to get these individuals moving better, more often, and with less discomfort.
References:
- Alrwaily M, Timko M, Schneider M, et al. Treatment-Based Classification System for Low Back Pain: Revision and Update. Physical Therapy. 2016;96(7):1057-1066.
- Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE. Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the maine lumbar spine study. Spine (Phila Pa 1976). Apr 15 2005;30(8):936-943.
- Belavý DL, Quittner MJ, Ridgers N, Ling Y, Connell D, Rantalainen T. Running exercise strengthens the intervertebral disc. Sci Rep. 2017 Apr;7 45975.
- Buchbinder R, van Tulder M, Öberg B, et al. Low back pain: a call for action. The Lancet. 2018;391(10137):2384-2388.
- Chou R, Deyo R, Friedly J, et al. Nonpharmacologic therapies for low back pain: a systematic review for an American College of Physicians clinical practice guideline. Ann Intern Med. 2017; 166:493-505.
- Current Concepts of Orthopaedic Physical Therapy 4th Ed. Orthopaedic Section, APTA, Inc.; 2016.
- Delitto A, Erhard RE, Bowling RW. A treatment-based classification approach to low back syndrome: identifying and staging patients for conservative treatment. Phys Ther. 1995 Jun;75(6):470-85; discussion 485-9.
- Delitto A, George SZ, Van Dillen L, Whitman JM, Sowa G, Shekelle P, Denninger TR, Godges JJ; Orthopaedic Section of the American Physical Therapy Association. Low back pain. J Orthop Sports Phys Ther. 2012 Apr;42(4):A1-57.
- Findlay GF, Hall BI, Musa BS, Oliveria MD, Fear SC. A 10-year follow-up of the outcome of lumbar microdiscectomy. Spine 1998; 23:1168–71.
- Flynn TW, Smith B, Chou R. Appropriate Use of Diagnostic Imaging in Low Back Pain: A Reminder That Unnecessary Imaging May Do as Much Harm as Good. J Orthop Sports Phys Ther. 2011;41(11):838-846.
- Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. The Lancet. 2018;391(10137):2368-2383.
- Fritz JM, Cleland JA, Childs JD. Subgrouping Patients With Low Back Pain: Evolution of a Classification Approach to Physical Therapy. J Orthop Sports Phys Ther. 2007;37(6):290-302.
- Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. The Lancet. 2018;391(10137):2356-2367.
- Karel YHJM, Verkerk K, Endenburg S, Metselaar S, Verhagen AP. Effect of routine diagnostic imaging for patients with musculoskeletal disorders: A meta-analysis. European Journal of Internal Medicine. 2015;26(8):585-595.
- Louw A, Diener I, Butler DS, Puentedura EJ. The Effect of Neuroscience Education on Pain, Disability, Anxiety, and Stress in Chronic Musculoskeletal Pain. Archives of Physical Medicine and Rehabilitation. 2011;92(12):2041-2056.
- Louw A, Zimney K, Puentedura EJ, Diener I. The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Physiotherapy Theory and Practice. 2016;32(5):332-355.
- Lurie JD, Birkmeyer NJ, Weinstein JN. Rates of advanced spinal imaging and spine surgery. Spine (Phila Pa 1976). 2003 Mar 15;28(6):616-20.
- Moseley GL, Butler DS. Fifteen Years of Explaining Pain: The Past, Present, and Future. The Journal of Pain. 2015;16(9).
- O’Connell NE, Cook CE, Wand BM, Ward SP. Clinical guidelines for low back pain: a critical review of consensus and inconsistencies across three major guidelines. Best Pract Res Clin Rheumatol. 2016; 30:968-980.
- O’Connell NE, Ward SP. Low Back Pain: What Have Clinical Guidelines Ever Done for Us? J Orthop Sports Phys Ther. 2018;48(2):54-57.
- Oliveira CB, Maher CG, Pinto RZ, et al. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. European Spine Journal. 2018;27(11):2791-2803.
- Puentedura EJ, Flynn T. Combining manual therapy with pain neuroscience education in the treatment of chronic low back pain: A narrative review of the literature. Physiotherapy Theory and Practice. 2016;32(5):408-414.
- Qaseem A, Wilt TJ, McLean RM, Forciea MA, Clinical Guidelines Committee of the American College of Physicians. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017; 166:514-530.
- Tousignant-Laflamme Y, Longtin C, Brismée J-M. How radiological findings can help or hinder patients’ recovery in the rehabilitation management of patients with low back pain: what can clinicians do? Journal of Manual & Manipulative Therapy. 2017;25(2):63-65.
- Yorimitsu E, Chiba K, Toyama Y, et al. Long term outcomes of standard discectomy for Lumbar Disc Herniation. Spine 2001;26:652– 8.
