The majority of individuals who come to physical therapy for a recent episode of low back pain have an excellent prognosis. In other words, there is a good chance that they will get better over time with the help of low-risk treatments such as physical therapy, non-steroidal anti-inflammatory drugs (NSAIDs) and early return to work and activity (DeLitto, 2012, Foster, 2018, Oliveira, 2018).
Our best available research evidence and expert clinical opinion in treating low back pain has these recommendations:

Seeing a physical therapist (PT) first before seeing a different health care provider (physician, chiropractor, orthopedic doctor etc.) has been shown to be quite helpful by:
- Lowering opiate use (Frogner, 2018)
- Reducing overutilization of imaging (Frogner, 2018)
- Improved Functional Outcomes & Fewer overall PT visits (Hon, 2020)
- Lowering overall cost of healthcare
- Seeing a PT first for neck or back pain, patients saved an average of $1,543! (Denninger, 2018)
- Seeing a PT first reduced overall cost and cost for PT (vs. seeing a physician first) for “musculoskeletal pain” (Hon, 2020)
- Seeing a PT first for back pain, patients had “significantly less out-of-pocket costs” (Frogner, 2018)
- Seeing a PT first vs. getting advanced imaging (MRI or CT scan) first saved patients an average of $4,753 over the course of the year on medical treatment costs! (Fritz, 2015)
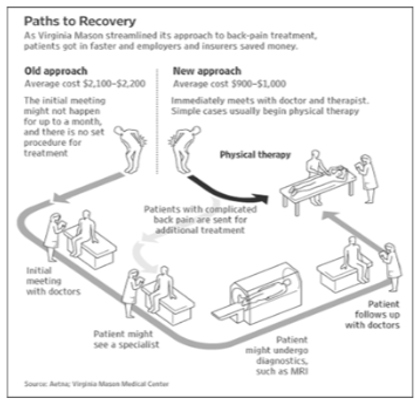
- Seeing a PT first for back pain, patients saved > $1,000 (Fuhrman, 2007) See Graphic Below:
Because all 50 states have legalized “Direct Access” (i.e., it is legal to see a physical therapist without having a referral from a doctor), it is increasingly important that PTs be confident and competent in performing medical screening for patients with low back pain to rule out the presence of serious spinal pathology before treating them.
*Note: Direct Access laws vary by state, see figure below:
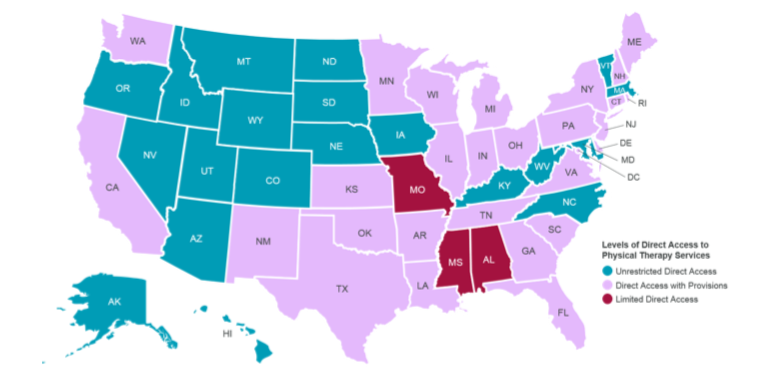
Image above from APTA.org Direct Access By State (Current as of Feb 2021; Accessed January 15th, 2022))
Part of our responsibility as frontline healthcare providers includes screening for “Red Flags” or possible indications of more serious spinal pathology.
I wanted to share some resources that I have been using in my clinical practice and sharing with physical therapy students through my teaching. Here are two keys that have informed the way that I prioritize medical screening for individuals with low back pain.
- Have a systematic way to screen
- Communicate your findings (with patient and provider)
1. Have a systematic way to screen
It is important to utilized screening methods that yield important results clinically and that are supported by research for their predictive power (i.e., factors that increase or decrease the likelihood that a pathology is present). Due to the high number of “Red Flag” signs and symptoms described for certain types of serious pathology, red flags have come under criticism if used alone or relied on without carefully scrutinizing their accuracy (Cook, 2018; Galliker, 2019; Verhagen, 2017).
An updated framework for screening decisions was developed by The International Federation of Orthopaedic Manipulative Physical Therapists (IFOMPT) and described in a recent 2020 article (Finucane, 2020). This framework recommends a three-step process that I have depicted below that seeks to provide practical steps to guide clinical decision making in physical therapy practice.
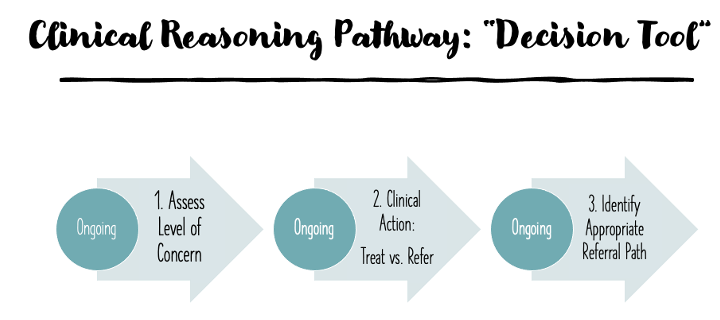
See my recent lecture on medical screening for low back pain for more on this decision tool and its use in PT practice.
Medical Screening for Low Back Pain Videos:
PT Medical Screen Lumbar Spine (Part 1):
PT Medical Screen Lumbar Spine (Part 2):
PT Medical Screen Lumbar Spine (Part 3):
2. Communicate your findings (with patient and provider)
Performing a thorough examination including subjective questioning and objective testing is of utmost importance in PT medical screening. After this has been done and the PT has synthesized the findings from this examination, the next stage is communicating these findings to the patient and also to other members of the healthcare team if appropriate.
The patient must be empowered to take an active role in their treatment, whether that is PT or seeking care elsewhere. Also, if the possibility of more serious pathology is present from exam findings, the patient must be educated on what to do if symptoms worsen—who to go see and how urgently this needs to be done.
Some tools that can aid in this communication process are called “Patient Scorecards” and below are examples of these that have been developed for cauda equina syndrome and spinal malignancy (cancer):
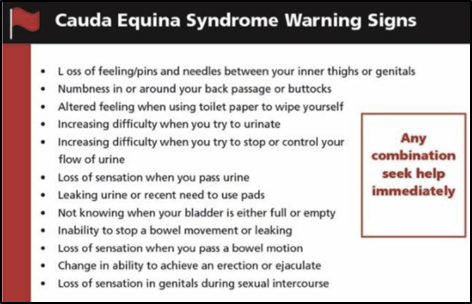
(Figure Above from: Greenhalgh, 2018)
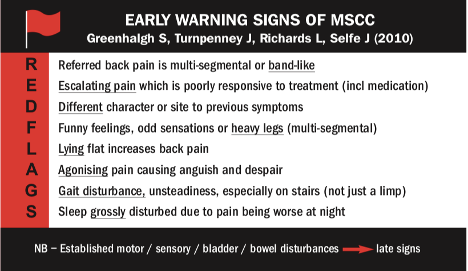
(Figure Above from: Turnpenny, 2015)
Stay Tuned for my upcoming post where I will discuss more about the most effective treatments for individuals with low back pain including physical therapy treatment strategies once a patient has been taken through the screening process and is deemed appropriate for PT intervention.
For more on these topics, check out my recent recorded lectures on Medical screening for the lumbar spine (Part 1) (Part 2) (Part 3) and also PT medical screening for rheumatic disease (Part 1) and (Part 2).
References:
Cook CE, George SZ, Reiman MP. Red flag screening for low back pain: nothing to see here, move along: a narrative review. Br J Sports Med. 2018;52(8):493-496.
Delitto A, George SZ, Van Dillen L, et al. Low Back Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. Journal of Orthopaedic & Sports Physical Therapy. 2012;42(4):A1-A57.
Denninger TR, Cook CE, Chapman CG, McHenry T, Thigpen CA. The Influence of Patient Choice of First Provider on Costs and Outcomes: Analysis From a Physical Therapy Patient Registry. J Orthop Sports Phys Ther. 2018;48(2):63-71.
Finucane LM, Downie A, Mercer C, et al. International Framework for Red Flags for Potential Serious Spinal Pathologies. J Orthop Sports Phys Ther. 2020;50(7):350-372.
Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. The Lancet. 2018;391(10137):2368-2383.
Fritz JM, Brennan GP, Hunter SJ. Physical Therapy or Advanced Imaging as First Management Strategy Following a New Consultation for Low Back Pain in Primary Care: Associations with Future Health Care Utilization and Charges. Health Serv Res. 2015;50(6):1927-1940.
Frogner BK, Harwood K, Andrilla CHA, Schwartz M, Pines JM. Physical Therapy as the First Point of Care to Treat Low Back Pain: An Instrumental Variables Approach to Estimate Impact on Opioid Prescription, Health Care Utilization, and Costs. Health Services Research. Published online May 23, 2018.
Fuhrmans, V. A Novel Plan Helps Hospital Wean Itself Off Pricey Tests. Wall Street Journal. January 12th, 2007.
Galliker G, Scherer DE, Trippolini MA, Rasmussen-Barr E, LoMartire R, Wertli MM. Low Back Pain in the Emergency Department: Prevalence of Serious Spinal Pathologies and Diagnostic Accuracy of Red Flags. The American Journal of Medicine. 2020;133(1):60-72.e14.
Greenhalgh S, Finucane L, Mercer C, Selfe J. Assessment and management of cauda equina syndrome. Musculoskeletal Science and Practice. 2018;37:69-74.
Hon S, Ritter R, Allen DD. Cost-Effectiveness and Outcomes of Direct Access to Physical Therapy for Musculoskeletal Disorders Compared to Physician-First Access in the United States: Systematic Review and Meta-Analysis. Phys Ther. 2020 Nov 27:pzaa201.
Oliveira CB, Maher CG, Pinto RZ, Traeger AC, Lin CC, Chenot JF, van Tulder M, Koes BW. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. Eur Spine J. 2018 Nov;27(11):2791-2803.
Turnpenney J, Greenhalgh S, Richards L, Crabtree A, Selfe J. Developing an early alert system for metastatic spinal cord compression (MSCC): Red Flag credit cards. Prim Health Care Res Dev. 2015;16(01):14-20.
Verhagen AP, Downie A, Maher CG, Koes BW. Most red flags for malignancy in low back pain guidelines lack empirical support: a systematic review. PAIN. 2017;158(10):1860-1868.

One Comment Add yours