
As many of the best clinicians (PTs, MDs, etc.) and current research suggest, shoulder pain that happens without acute trauma (i.e., more likely due to “overuse”) very often responds well to conservative, non-surgical treatments like physical therapy.
There have been different names given to this type of shoulder pain and some are based on theories for a specific “tissue” (i.e., muscle, tendon, bursa, bone) that is injured or irritated. However, just like with most non-traumatic low back pain, “tissue-based” diagnoses can fall short of fully explaining the cause of pain in the shoulder (Diercks, 2014; Innocenti, 2019). Additionally, a high percentage of individuals with NO shoulder pain have been found to have tissues that are “injured” when imaging is performed (i.e., evidence of rotator cuff pathology, labral tears, etc. on X-ray or MRI) See: You Are Not Your X-Ray . This makes the case to view this type of shoulder pain as pretty non-specific, whether we call it “non-traumatic shoulder pain,” “rotator-cuff related shoulder pain,” or the commonly used “subacromial impingement syndrome.”
Should we view “Rotator-Cuff Related Shoulder Pain” as the newest “Non-Specific Low Back Pain”?
Leda McDaniel, PT, DPT, OCS
Despite this shortcoming, it is helpful to have some sense of the common diagnostic terminology and how it is commonly used. See below for a quick break-down of common (non-traumatic) shoulder diagnoses:
- “Rotator-Cuff Related Shoulder Pain” (aka, “Rotator Cuff Injury”, “Rotator Cuff Tear”) (Doiron-Cadrin, 2020; Lewis, 2016): This is a “catch-all” broad category that includes partial or full rotator cuff tear, rotator cuff tendinopathy and even “shoulder impingement” at its broadest definition!
- “Subacromial Impingement Syndrome” (aka “Shoulder Impingement”) (Pieters, 2020): originally proposed diagnostic term based on the theory that a certain type of shoulder pain was due to “impingement” of structures in the subacromial space (could include rotator cuff tendons, subacromial bursa, long head of biceps tendon, etc.)
When an individual comes in for a physical therapy evaluation with shoulder pain and does NOT have a single traumatic event that caused it (i.e., falling, catching oneself in an awkward position, getting hit in the shoulder, etc.), I will usually recommend and find success in treating their shoulder with a combination of exercise-based treatments and some hands-on treatment (i.e., manual therapy).
Patients may get pain relief from ice or over the counter NSAIDs medications, but very rarely have I seen this type of shoulder pain require more aggressive forms of treatment like surgery or a steroid injection. Research also supports these approaches, especially exercise-based treatments, as they have been consistently recommended from “Clinical Practice Guidelines” for shoulder pain (Doiron-Cadrin, 2020) and have been found to have high levels of success for this type of shoulder pain by improving long-term pain, mobility (i.e., range of motion), and physical function (Pieters, 2020). Also, systematic reviews give a strong recommendation AGAINST SURGERY (i.e., “subacromial decompression surgery”) as a treatment for “subacromial” or “non-traumatic” shoulder pain (Barrett, 2020; Vandvik, 2019), reminding us that surgery may confer added risks and may not lead to an improvement in pain, function, or quality of life .
As tempting as it might be to turn to other more “passive” treatment options like laser, ultrasound, or injections for a “quick-fix” solution, the best research evidence (and from what I’ve seen in my clinical practice) does not support using these modalities as stand-alone treatments (it is questionable even to add them to other treatments) (Doiron-Cadrin, 2020; Pieters, 2020).
Manual therapy is often recommended, though again usually not as a stand-alone treatment, and the effectiveness or superiority of specific types of manual therapy are uncertain (Doiron-Cadrin, 2020; Innocenti, 2019; Pieters, 2020).
So, if exercise is our top choice, what are the best exercises to use for shoulder rehab? Well, likely there will be a progression of loading based on symptom irritability. See Figure Below for a general idea of how to progress loading in rehabilitation settings (for suspected tendon/muscle pathology):

Even if we think that exercise should be helpful, the best types of exercises to improve “non-traumatic shoulder pain” have not been established. (Dube, 2020). A review investigating eccentric exercises did not find a difference between this and other types of exercise for “subacromial impingement” (Larsson, 2019). Furthermore, it has not been well established, why exercise improves this type of shoulder pain!
The tendency may be to theorize that “strengthening” provides the noted improvement we often see from exercise. One narrative review seems to argue against this idea, stating: “The rationale for prescribing resistance exercise for nontraumatic RCRSP (“Rotator-Cuff Related Shoulder Pain”) needs to be reframed as a multidimensional intervention that can confer benefit by numerous interrelated biopsychosocial processes, not simply by increasing shoulder strength or improving shoulder mechanics.” (Powell, 2021)
Given the findings above, it still may be wise to select exercises that target muscles that surround the shoulder and shoulder blade independent of mechanism of action. Perhaps we are improving “load-tolerance” of the shoulder, much like how we discuss treatment for tendinopathy? In any case, I still feel that selection of exercises that have high recruitment from muscles impacting the shoulder (rotator cuff: supraspinatus, infraspinatus, teres minor, subscapularis) and shoulder blade (e.g., trapezius, rhomboids, levator scapula, teres major, latissimus dorsi etc.) may be helpful to integrate.
See this post: Best Shoulder and Scapula Exercises for exercises that have demonstrated high EMG recruitment from specific rotator cuff and scapular muscles (or checkout this downloadable PDF Table: Best Shoulder & Scapula Exercises)

Another great resource is the “Thrower’s Ten” Program, which has been used as a comprehensive shoulder/arm strengthening program for athletes (especially for throwing athletes), and can be a useful guide of exercises to incorporate in shoulder rehabilitation (originally described in Wilk, 1997). It has shown to improve upper extremity strength and power in various populations (Escamilla, 2011; Gokalp, 2020;).
Iterations of the original thrower’s ten program include the “Advanced” version integrating core control and stability demands (Wilk, 2011) and a version for youth athletes using bands and body weight resistance (Wilk, 2021). See Below for the original Thrower’s Ten Program:
THROWER’S TEN PROGRAM (From Dr. James Andrews Center’s Website: https://www.andrewssportsmedicine.com
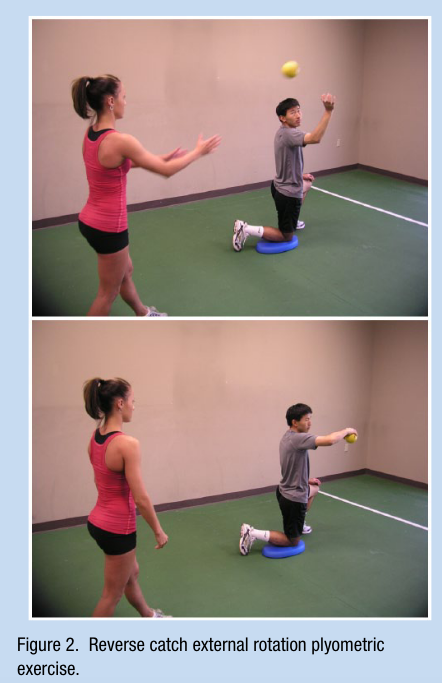
Later in rehabilitation, it can be helpful to include exercises that necessitate more dynamic control at the shoulder and improve power production (i.e., “upper extremity” plyometrics). Two of the exercises that have been shown to be most impactful on functional strength and power development are an external rotation deceleration drill and a prone ball drop and catch drill with the shoulder at 90 degrees of abduction and the elbow at 90 degrees of flexion (i.e., “the 90/90 position”) (See Pictures Below of these exercises and See Carter, 2007 and Ellenbecker, 2015 references below for more detailed discussion of how to implement these exercises and dosing).

I hope this post helps with rationale for exercise selection for “non-traumatic shoulder pain”. Please feel free to comment below with any questions!
References:
SapiensMoves Blog Post on Shoulder/Scapula Exercises:
Barrett E, Larkin L, Caulfield S, de Burca N, Flanagan A, Gilsenan C, Kelleher M, McCarthy E, Murtagh R, McCreesh K. Physical Therapy Management of Nontraumatic Shoulder Problems Lacks High-Quality Clinical Practice Guidelines: A Systematic Review With Quality Assessment Using the AGREE II Checklist. J Orthop Sports Phys Ther. 2021 Feb;51(2):63-71.
Carter AB, Kaminski TW, Douex AT Jr, Knight CA, Richards JG. Effects of high-volume upper extremity plyometric training on throwing velocity and functional strength ratios of the shoulder rotators in collegiate baseball players. J Strength Cond Res. 2007 Feb;21(1):208-15.
Diercks R, Bron C, Dorrestijn O, Meskers C, Naber R, de Ruiter T, Willems J, Winters J, van der Woude HJ; Dutch Orthopaedic Association. Guideline for diagnosis and treatment of subacromial pain syndrome: a multidisciplinary review by the Dutch Orthopaedic Association. Acta Orthop. 2014 Jun;85(3):314-22.
Doiron-Cadrin P, Lafrance S, Saulnier M, Cournoyer É, Roy JS, Dyer JO, Frémont P, Dionne C, MacDermid JC, Tousignant M, Rochette A, Lowry V, Bureau NJ, Lamontagne M, Coutu MF, Lavigne P, Desmeules F. Shoulder Rotator Cuff Disorders: A Systematic Review of Clinical Practice Guidelines and Semantic Analyses of Recommendations. Arch Phys Med Rehabil. 2020 Jul;101(7):1233-1242.
Dubé MO, Desmeules F, Lewis J, Roy JS. Rotator cuff-related shoulder pain: does the type of exercise influence the outcomes? Protocol of a randomised controlled trial. BMJ Open. 2020 Nov 5;10(11):e039976.
Ellenbecker TS, Sueyoshi T, Bailie DS. Muscular activation during plyometric exercises in 90° of glenohumeral joint abduction. Sports Health. 2015 Jan;7(1):75-9.
Escamilla RF, Ionno M, deMahy S, et al. Comparison of three baseballspecific six-week training programs on throwing velocity in high school baseball players. Med Sci Sports Exerc. 2011;43(5):836–837
Gokalp O, Kirmizigil B. Effects of Thrower’s Ten exercises on upper extremity performance: A randomized controlled study. Medicine (Baltimore). 2020 Oct 16;99(42):e22837.
Innocenti T, Ristori D, Miele S, Testa M. The management of shoulder impingement and related disorders: A systematic review on diagnostic accuracy of physical tests and manual therapy efficacy. Journal of Bodywork and Movement Therapies. 2019;23(3):604-618.
Larsson R, Bernhardsson S, Nordeman L. Effects of eccentric exercise in patients with subacromial impingement syndrome: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2019 Oct 14;20(1):446.
Lewis J. Rotator cuff related shoulder pain: Assessment, management, and uncertainties. Man Ther. 2016 Jun;23:57-68.
Pieters L, Lewis J, Kuppens K, Jochems J, Bruijstens T, Joossens L, Struyf F. An Update of Systematic Reviews Examining the Effectiveness of Conservative Physical Therapy Interventions for Subacromial Shoulder Pain. J Orthop Sports Phys Ther. 2020 Mar;50(3):131-141.
Powell JK, Lewis JS. Rotator Cuff–Related Shoulder Pain: Is It Time to Reframe the Advice, “You Need to Strengthen Your Shoulder”? J Orthop Sports Phys Ther. 2021;51(4):156-158.
Vandvik PO, Lähdeoja T, Ardern C, Buchbinder R, Moro J, Brox JI, Burgers J, Hao Q, Karjalainen T, van den Bekerom M, Noorduyn J, Lytvyn L, Siemieniuk RAC, Albin A, Shunjie SC, Fisch F, Proulx L, Guyatt G, Agoritsas T, Poolman RW. Subacromial decompression surgery for adults with shoulder pain: a clinical practice guideline. BMJ. 2019 Feb 6;364:l294.
Wilk KE, Andrews JR, Arrigo CA, et al. Preventive and Rehabilitative Exercises for the Shoulder and Elbow. 5th ed. Birmingham, AL: American Sports Medicine Institute; 1997.
Wilk KE, Lupowitz LG, Arrigo CA. The Youth Throwers Ten Exercise Program: A variation of an exercise series for enhanced dynamic shoulder control in the youth overhead throwing athlete. Int J Sports Phys Ther. 2021.
Wilk KE, Yenchak AJ, Arrigo CA, Andrews JR. The Advanced Throwers Ten Exercise Program: a new exercise series for enhanced dynamic shoulder control in the overhead throwing athlete. Phys Sportsmed. 2011 Nov;39(4):90-7.
