One of my specialty interests in physical therapy is teaching about pain science principles and also integrating these principles in my physical therapy practice when working with patients with persistent pain (and really all pain!). As I seek to practice in the most effective manner, but also communicate some of these principles, I am often struck by how much language influences beliefs, which influences behavior…which influences activity choices and quality of life and emotions and on and on…
What I am trying to say is language is POWERFUL! The words that we use can make a huge impact on our patients’ activity choices, belief in their abilities, and healing and recovery potential.
This leads me to really emphasize in my teaching and my work with patients the use of positive language and framing when talking about injury and recovery. It truly is amazing how adaptable we are as human beings and the body’s innate abilities to heal and recover. I also am very passionate about trying to stay away from language that can potentially cause harm (i.e., “nocebo” or “nocebic” language) and language that overemphasizes “pathoanatomical” causes as the ONLY potential cause of pain or injury (For more on this see: “You Are NOT Your X-Ray”).
A great way to focus on the positive aspects of injury recovery is to remember that the body has an AMAZING ability to heal and some of our newest evidence and research is supporting healing even in body areas that some believed to be unable to heal without surgical intervention. A few examples of this are spontaneous healing of lumbar disc herniations and ACL ruptures! Check out the articles that I have cited below if you want to learn more!
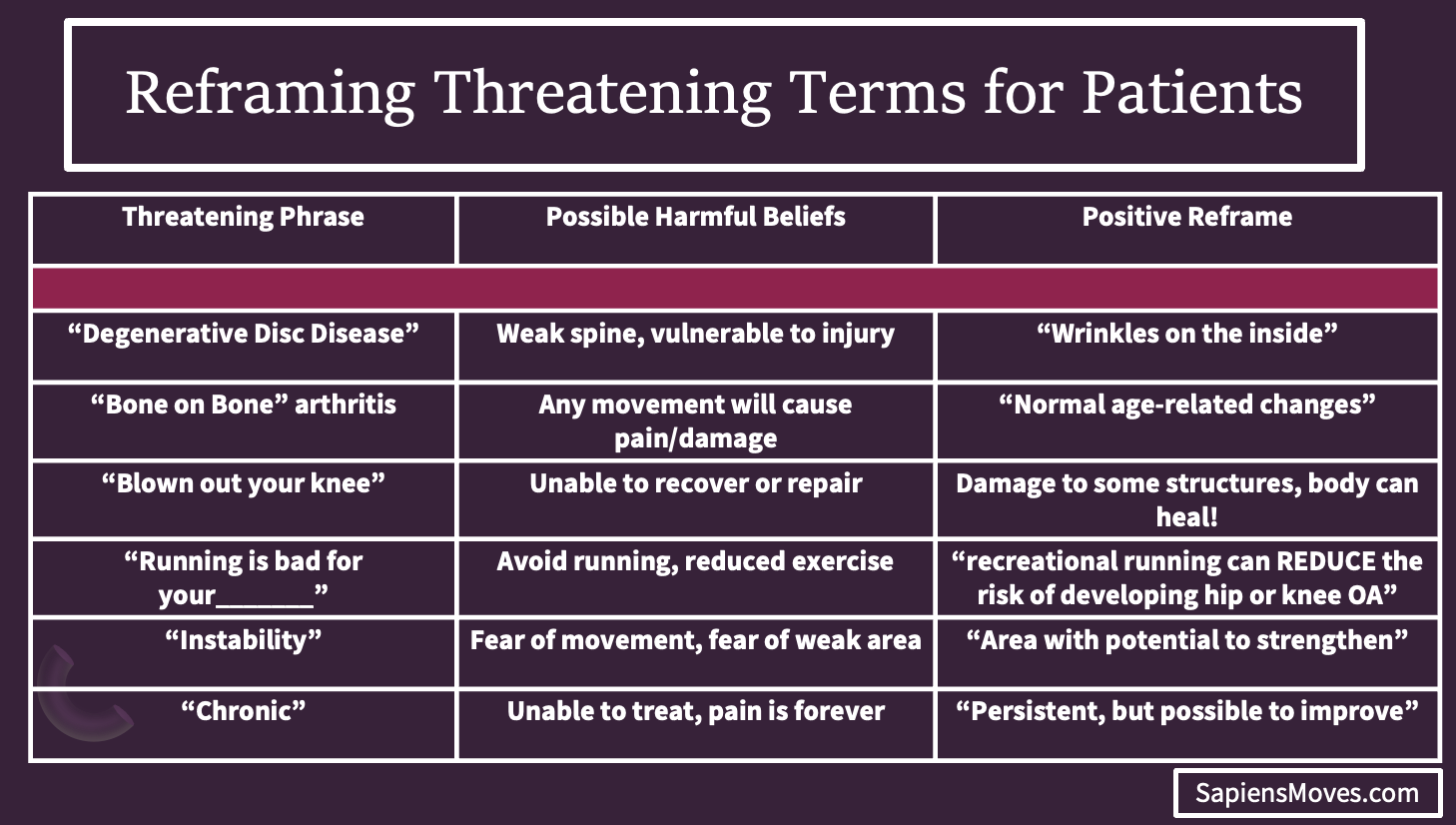
Also, If you are interested in some phrases to use that may replace “harmful” or fear inducing phrases (and may in fact be more truthful!) check out the table below:
Stay tuned for future posts on key pain science principles and a look at matching our treatments to an individual’s proposed pain “mechanism”…
References:
Importance of Language:
•Bedell SE, Graboys TB, Bedell E, Lown B. Words That Harm, Words That Heal. Archives of Internal Medicine. 2004;164:4.
•Stewart M, Loftus S. Sticks and Stones: The Impact of Language in Musculoskeletal Rehabilitation. Journal of Orthopaedic & Sports Physical Therapy. 2018;48(7):519-522.
Recreational Running Could be “protective”:
•Alexander JLN, Willy RW, Culvenor AG, Barton CJ. Infographic. Running Myth: recreational running causes knee osteoarthritis. Br J Sports Med. 2022;56(6):357-358.
Disc Healing:
•Jiang H. Incidence of Spontaneous Resorption ofLumbar Disc Herniation: A Meta-Analysis. Pain Phys. 2017;1(21;1):E45-E52. doi:10.36076/ppj.2017.1.E45
•Lee J, Ha IH, Kim M riong, et al. Pain, disability, and MRI changes in lumbar disc herniation patients treated with integrative medicine: Ten-year results of an observational study. Integrative Medicine Research. 2022;11(2):100833.
•Yu P, Mao F, Chen J, et al. Characteristics and mechanisms of resorption in lumbar disc herniation. Arthritis Res Ther. 2022;24(1):205.
ACL Healing:
•Costa-Paz M, Ayerza MA, Tanoira I, Astoul J, Muscolo DL. Spontaneous Healing in Complete ACL Ruptures: A Clinical and MRI Study. Clinical Orthopaedics & Related Research. 2012;470(4):979-985.
•Filbay SR, Roemer FW, Lohmander LS, Turkiewicz A, Roos EM, Frobell R, Englund M. Evidence of ACL healing on MRI following ACL rupture treated with rehabilitation alone may be associated with better patient-reported outcomes: a secondary analysis from the KANON trial. Br J Sports Med. 2023 Jan;57(2):91-98.
