“Can you treat my pain, or do I just have to learn to live with it?”
This is a question that I get a LOT as a physical therapist. Most of the patients that I see in physical therapy are coming in wondering how they can better control or alleviate their pain and if we can help identify what is causing the pain. As I work with these patients, I have found that having a better understanding of the neurobiology of pain (i.e., how our body and nervous system creates and processes threat and pain) and using simplified language and explanations of pain for their understanding of pain can really improve outcomes!
I am continually refining the language that I use to explain pain to patients and other healthcare professionals when I give lectures about pain science. I have found that the more that we can empower our patients with knowledge about how pain works, often the less pain they experience. Also, the more we can match our physical therapy treatments to a greater understanding of pain systems and mechanisms the more confident I am in telling my patients that, yes, we can reduce their pain and they won’t just have to, “learn to live with it.”
In this series of blog posts, I will cover some of explanations that I use with patients and practitioners about what pain is and how it functions to protect us and some tips on how to assess and treat pain in physical therapy practice.
Part 1: How to Talk to Patients in Pain
Language, whether implicit (body language) or explicit (words), communicates key messages to our patients in physical therapy sessions and can make a HUGE impact on our rapport with patients and also our outcomes! Bringing some awareness to how we communicate with our patients can enhance the patient experience and also help us to avoid potential negative effects from our interactions (i.e., “iatrogenic” or “nocebic”: harming effects). With this in mind, I’d like to quickly define some terms related to language and then dive into some pain-science informed recommendations for communicating with our patients in a physical therapy (and medical) setting!
Key Terms Defined:
Pain:
The definition of pain is complex and has been revised and refined over the years. The most up to date definition comes from The International Association for The Study of Pain and goes as follows (Raja, 2020; Treede, 2018):
“An aversive sensory and emotional experience, typically caused by, or resembling that caused by, actual or potential tissue damage” *
- *6 Notes clarify this definition and read as follows (Pain is always subjective, Pain is different than nociception, Pain is learned about through life experiences, A person’s report of pain should be accepted, Pain is usually protective, but experience of pain could harm function and/or social/psychological well-being, Pain may be experienced by humans and non-human animals)
Nociception:
The detection and transmission of sensory input from “nociceptors” or also known as danger receptors that detect three types of information: temperature, pressure (mechanical inputs), chemical inputs and send signals to the spinal cord and if appropriate up to the brain. Input from nociceptors can contribute to a person’s experience of pain but is not the same thing as pain. Nociception is a sensation vs. pain is a perceptual experience! See the table below for the differences between pain and nociception.
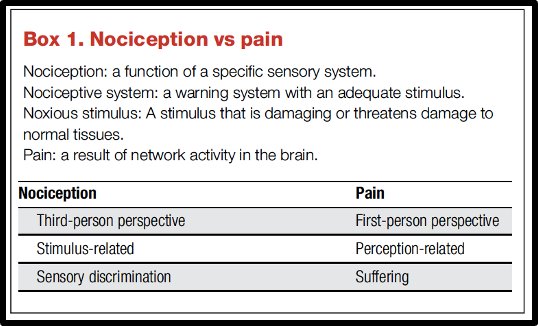
(Chart above from Treede, 2018)
Placebo:
From the Latin “placere” meaning to please, placebo effects often refer to noted impact or benefits from a substance or factor that does not have an active ingredient known to be beneficial.
Nocebo:
From the Latin “nocere” meaning “to harm”. Nocebo effects are substances or factors that harm an individual that do not contain active ingredients or are not in themselves inherently harmful.
As you may notice from the definition of pain above, tissue damage can be part of what causes pain, but even the threat of tissue damage could contribute to pain! This gets at the often-confusing concept that pain is not the same as tissue damage. Another example of this distinction, as I have written about before, is the high proportion of asymptomatic populations who have pathological imaging findings (e.g., spine disc bulges, hip and/or shoulder labral tears, etc.). So, as we see tissue injury is not necessary or sufficient (in all cases) to cause an automatic pain response.
A couple of helpful metaphors or pictures that I tend to use when talking about pain and working to improve health in my patients in physical therapy are:
- Pain as “an alarm signal”
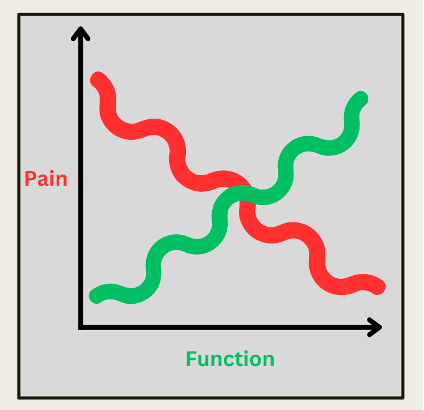
- Pain vs. Function Chart
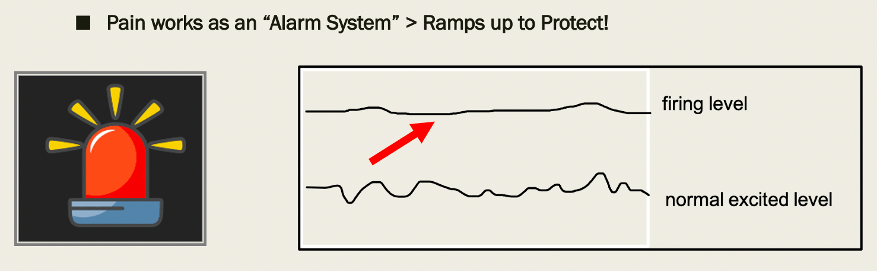
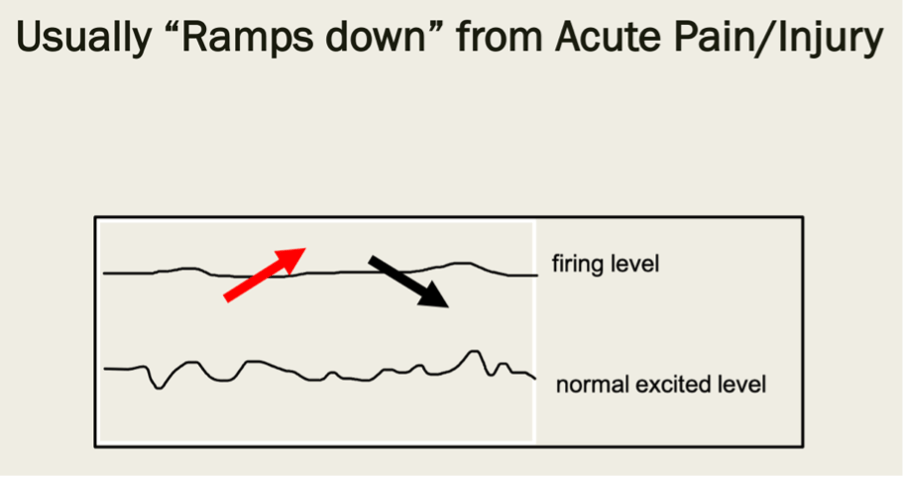
As the pictures above show, pain goes off like an alarm system to alert us of danger or call are attention to a place of injury so we can seek treatment. In this way, pain is protective and positive! But we want to make sure we try to address the source of the pain so that the alarm is effective and so that it turns off after it has served its function.
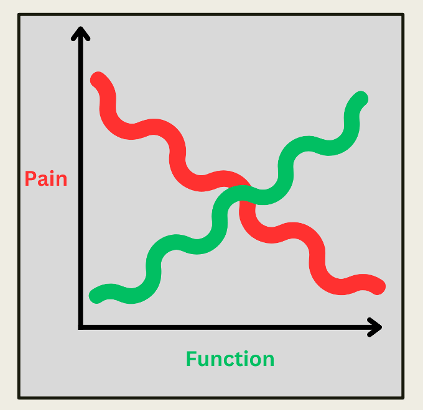
The picture above depicts recovery from injury or a standard rehabilitation process. As you can see from the picture, our goal (an expectation) is that pain will gradually decrease, and function will increase. However, as you notice from the chart, this process is not necessarily linear, and we may see an increase in function before we ever see a drop in pain! With this in mind, we want to not only focus on the goal of pain reduction, but also focus on improving function, movement, and activity too!
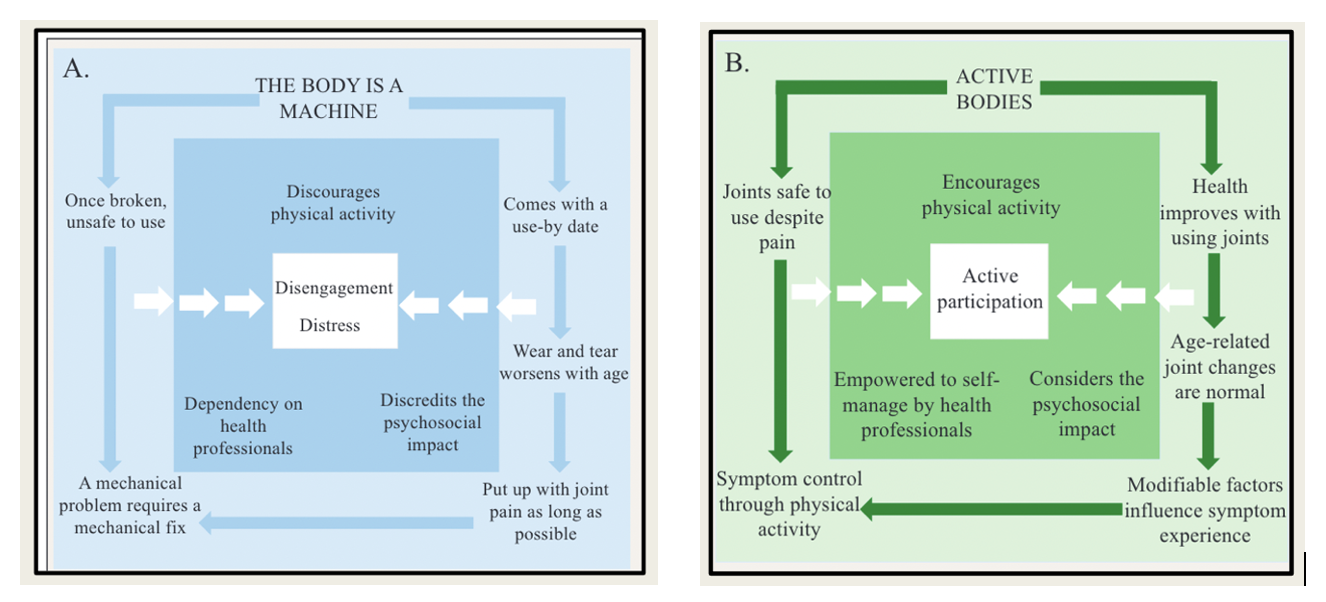
This concept is a key theme in a neat article that was published this year (Bunzli, 2023) called: “Broken Machines or Active Bodies? Part 2: How People Talk About Osteoarthritis and Why Clinicians Need to Change the Conversation” In the article, the authors discuss the narratives that individuals with knee osteoarthritis have for explaining their knee pain. One group tended to hold the view of “the body is a machine,” and along with this view came themes of joint destruction, pain equating to damage, and aging degeneration, which as you might expect led to more pain and less movement! A second group held the view and focus on “active bodies,” and had the perspectives of the body as adaptive, able to strengthen around the knee joint, and imaging findings as natural age-related changes. IN contrast, this second group was more active, despite some pain, and really lived out the “focus on function,” mentality!
As you can see, the language that we use to conceptualize pain, talk about its protective function, and educate our patients and colleagues about how it works within our nervous system are important! For more on the power of language and choosing helping and healthy language vs. harmful language, I highly recommend these articles:
Sticks and Stones: The Impact of Language in Musculoskeletal Rehabilitation
Words That Harm, Words That Heal
AND: Part 3 of the series, discussing treatment tips for complex pain presentations
References:
- Bedell SE, Graboys TB, Bedell E, Lown B. Words That Harm, Words That Heal. Archives of Internal Medicine. 2004;164:4.
- Bunzli S, Taylor NF, O’Brien P, et al. Broken Machines or Active Bodies? Part 2. How People Talk About Osteoarthritis and Why Clinicians Need to Change the Conversation. Journal of Orthopaedic & Sports Physical Therapy. 2023;53(6):325-330.
- Louw A. Why Do I Hurt? A Patient Book About The Neuroscience of Pain. Minneapolis, Minnesota: Orthopedic Physical Therapy Products; 2013.
- Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976-1982.
- Stewart M, Loftus S. Sticks and Stones: The Impact of Language in Musculoskeletal Rehabilitation. Journal of Orthopaedic & Sports Physical Therapy. 2018;48(7):519-522.
- Treede RD. The International Association for the Study of Pain definition of pain: as valid in 2018 as in 1979, but in need of regularly updated footnotes. PAIN Reports. 2018;3(2):e643.

2 Comments Add yours