
In this post I want to discuss 3 Keys to treatment for posterior thigh and buttock pain. If you are interested in differential diagnosis and screening for posterior thigh and buttock pain, please check out:
Part 1- Differential Diagnosis of Posterior Thigh and Buttock Pain
Three Treatment Keys:
- Correct Differential Diagnosis
- Activity Modifications & Reducing Symptom Aggravators
- Exercise Prescription & Progressions
1-Correct Differential Diagnosis
To have the best chance at treatment success, identifying the cause of symptoms is paramount! As discussed in the first post:
Part 1- Differential Diagnosis of Posterior Thigh and Buttock Pain
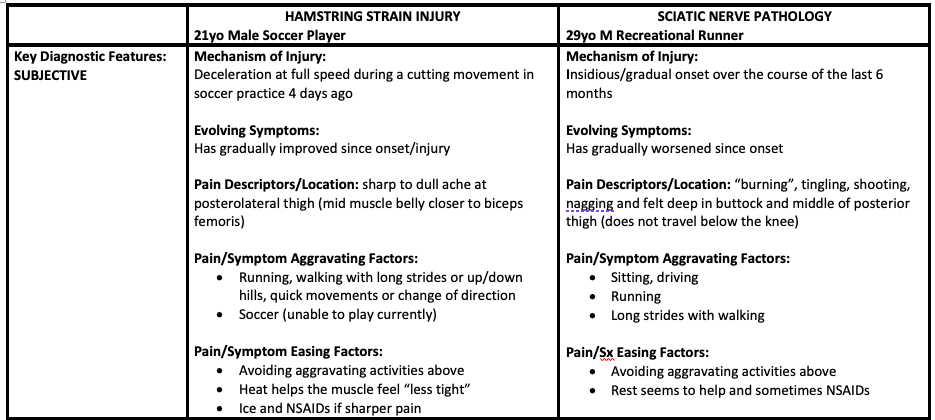
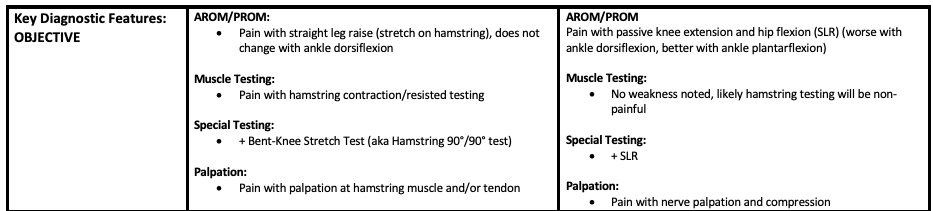
and in the case studies below, there are some important clues that are unique to hamstring injury vs. sciatic nerve irritation that should help you identify which is the potential cause of symptoms. It is also helpful when you are treating these injuries to further identify which part of this tissue is potentially injured or causing symptoms.
For Example:
Hamstring Injury:
- Which hamstring muscle is injured (semitendinosus, semimembranosus, biceps femoris)?
- What part of the muscle-tendon unit is injured (muscle belly vs. high hamstring tendon vs. musculotendinous junction)?
Sciatic Nerve:
- Is there a source of nerve compression?
- Is there a history of hamstring injury and potential scar tissue formation?
- Is there a contributor from the lumbar spine?
Once you have performed a thorough evaluation and have identified the area to treat and likely cause, you can start making treatment decisions:
2-Activity Modifications & Reducing Symptom Aggravators
Activity modification in the case of hamstring strain injury will largely depend on the grade or severity of injury. Higher grade (more severe) injuries may necessitate use of an assistive device like crutches for walking and weight bearing activities. Medium to low grade strains may respond well to a short break (2-4 weeks) from sports, running, and reducing stride length in walking if symptomatic.
Activity modification in the case of sciatic nerve injury will depend on the “irritability” of the injury (i.e., how much stress/activity it takes to cause symptoms and how long symptoms take to calm down). Likely modifications will be to avoid positions of “neural tension” such as a straight leg forward bend/toe touch motion and straight leg kicking up. It would also be wise to avoid or reduce frequency of any aggravating exercise related activities as symptoms are allowed to calm down. This could include running, sports, or fast walking.
3-Exercise Prescription & Progressions
Exercise prescription for hamstring strain injury will typically follow a staged progression depending on severity of injury and stage of healing from time of injury. With low grade injuries (e.g., grade I), individuals may tolerate immediate introduction of low load isotonic exercises (concentric and eccentric) such as open chain hamstring curls or deadlift variations. If the injury is more severe, (e.g., grade III), individuals may be started on submaximal (e.g., 25-50% effort) multiangle hamstring isometrics if tolerated and utilize a “pain monitoring model” with exercises. Progression of load will be gradual as strength and motor control improves and symptoms decrease. Ultimately, the goal would be to introduce higher-level eccentric exercises (see below for examples and evidence-based choices for hamstring exercises!). It will be important to avoid stretching early on as this can exacerbate symptoms.
Including eccentric, “lengthening” exercises in hamstring rehabilitation has been shown to reduce time for returning to sport compared with rehabilitation with “standard” hamstring exercises (Askling, 2013) :
“Lengthening Hamstring Exercises” (See Pictures Below):
- “Extender” Exercise
- “Diver” Exercise
- “Glider” Exercise
VS.
“Standard Hamstring Exercises”:
- Hamstring Stretch (contract/relax)
- Single Leg Bridge Exercise
- Hip Extension (Cable Pull) Exercise

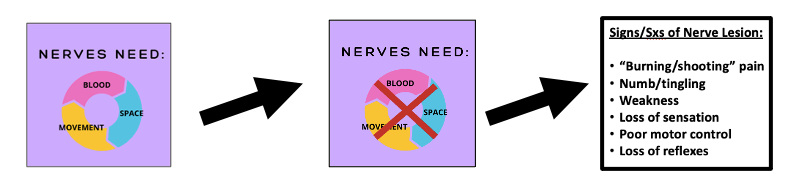
Exercise prescription for sciatic nerve pathology is more variable depending on the cause of symptoms (e.g., compression, tension, general “irritation”). But, treatment will likely include exercises or manual therapy techniques matched to the proposed cause of irritation (e.g., compression, stretch positions, hypoxia of tissues). Healthy nerves respond well when given “space, movement, and blood” and treatments can line up with these principles to promote nerve health and reduce irritation. It will be important to avoid stretching or “tensioning” the nerve early on as this could exacerbate symptoms. Aerobic exercise serves as the basis for treatment (as long as non-symptom provoking) because of its overall contribution to blood flow and oxygen distribution, which will facilitate healing and likely reduce pain via exercise-induced analgesia. Low-intensity aerobic exercise choices that my be beneficial include stationary bicycle, walking (short strides), swimming or water aerobics, and/or light yoga in pain free positions.
It will likely be helpful to avoid long durations of sitting (due to compression) and crossing of the legs or prolonged internal rotation at the hip because of the tension created in the sciatic nerve with these positions. Later stages of rehabilitation when irritability of symptoms is reduced, could include the introduction of some “tensioner” type neurodynamic treatment techniques. Possible adjunct treatments to physical therapy exercises and manual therapy-based treatments could include the use of NSAIDs or neuropathic pain medications such as gabapentin or pregabalin (Park, 2020).
Recap of Diagnostic Rationale for Nerve Injury/Pathology:
See figure below for examples of physical therapy neurodynamic treatment approaches (Matched to Proposed Mechanism):
Finally, check out the two case studies below that describe some of the key differences between testing and treatment of hamstring related injury vs. sciatic nerve related injury.

References:
Askling CM, Tengvar M, Thorstensson A. Acute hamstring injuries in Swedish elite football: A prospective randomised controlled clinical trial comparing two rehabilitation protocols. British Journal of Sports Medicine. 2013;47(15):953-959.
Cyriax J. Textbook of orthopaedic medicine, diagnosis of soft tissue lesions, vol 1, 8th edition. London: Baillière Tindall; 1982.
Current Concepts of Orthopaedic Physical Therapy 4th Ed.Orthopaedic Section, APTA, Inc.; 2016.
De Ridder R, De Blaiser C, Verrelst R, De Saer R, Desmet A, Schuermans J. Neurodynamic sliders promote flexibility in tight hamstring syndrome. European Journal of Sport Science. Published online October 22, 2019:1-8.
Erickson LN, Sherry MA. Rehabilitation and return to sport after hamstring strain injury. Journal of Sport and Health Science. 2017;6(3):262-270.
Heiderscheit BC, Sherry MA, Silder A, Chumanov ES, Thelen DG. Hamstring Strain Injuries: Recommendations for Diagnosis, Rehabilitation, and Injury Prevention. Journal of Orthopaedic & Sports Physical Therapy. 2010;40(2):67-81.
Laslett M, Aprill CN, McDonald B, Young SB. Diagnosis of Sacroiliac Joint Pain: Validity of individual provocation tests and composites of tests. Manual Therapy. 2005;10(3):207-218.
Laslett M, Young SB, Aprill CN, McDonald B. Diagnosing painful sacroiliac joints: A validity study of a McKenzie evaluation and sacroiliac provocation tests. Australian Journal of Physiotherapy. 2003;49(2):89-97.
López López L, Torres JR, Rubio AO, Torres Sánchez I, Cabrera Martos I, Valenza MC. Effects of neurodynamic treatment on hamstrings flexibility: A systematic review and meta-analysis. Physical Therapy in Sport. 2019;40:244-250.
Maitland G; Hengeveld E, Banks K, eds. Maitland’s Vertebral Manipulation: Management of Neuromusculoskeletal Disorders—Volume 1. 8th ed. London, United Kingdom: Churchill Livingstone; 2013.
Martin HD, Khoury A, Schröder R, Palmer IJ. Ischiofemoral Impingement and Hamstring Syndrome as Causes of Posterior Hip Pain. Clinics in Sports Medicine. 2016;35(3):469-486.
Martin RL, Schröder RG, Gomez-Hoyos J, et al. Accuracy of 3 Clinical Tests to Diagnose Proximal Hamstrings Tears With and Without Sciatic Nerve Involvement in Patients With Posterior Hip Pain. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2018;34(1):114-121.
Park JW, Lee YK, Lee YJ, Shin S, Kang Y, Koo KH. Deep gluteal syndrome as a cause of posterior hip pain and sciatica-like pain. Bone Joint J. 2020 May;102-B(5):556-567.
Robinson DR. Pyriformis syndrome in relation to sciatic pain. The American Journal of Surgery. 1947;73(3):355-358
Sherry MA, Best TM. A Comparison of 2 Rehabilitation Programs in the Treatment of Acute Hamstring Strains. RESEARCH REPORT. 2004;34(3):10.
Telli H, Telli S, Topal M. The Validity and Reliability of Provocation Tests in the Diagnosis of Sacroiliac Joint Dysfunction. Pain Physician. 2018 Jul;21(4):E367-E376. PMID: 30045603.
van der Wurff P, Buijs EJ, Groen GJ. A Multitest Regimen of Pain Provocation Tests as an Aid to Reduce Unnecessary Minimally Invasive Sacroiliac Joint Procedures. Archives of Physical Medicine and Rehabilitation. 2006;87(1):10-14..

One Comment Add yours