
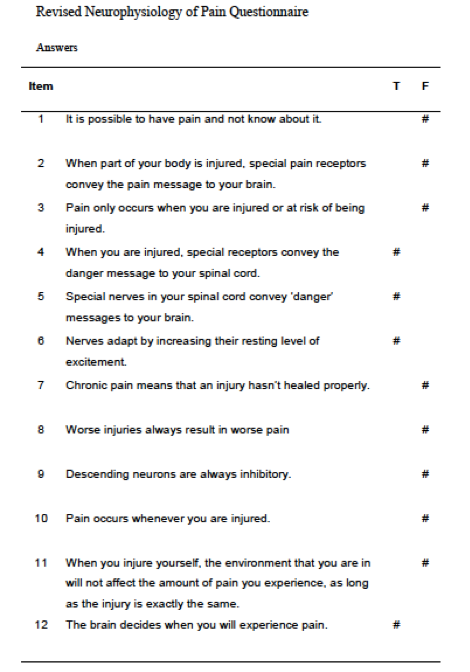
If you are a physical therapist, doctor, nurse—really any healthcare professional, you will agree with me that pain is EVERYWHERE! It is part of the human experience to feel pain and pain is one of the main reasons that patients come to physical therapy1. If pain is so common and if pretty much all the patients that you are working with have it, how much do you really know about pain? Feel free to test yourself by taking the quiz below (answers at the end of this post)2

As part of your patient education, there may be many reasons to include education on pain:
· Pain can be used as a proxy for “load tolerance” 3,4 and can guide rehabilitation exercise dosing prescriptions. For example, Silbernagel et al. (2001)3 use a pain monitoring model to guide Achilles’ tendinopathy rehabilitation. See figure below:

(Figure from Silbernagel et al., 2001)3
· Pain location may help in differential diagnosis5: but remember pain is just one part of a comprehensive clinical picture including history, comorbidities, strength, mobility…
· Pain quality and severity can indicate stage of healing5: For example, sharp and high intensity pain is more indicative of an acute/inflammatory stage vs. dull, aching pain may be more common in proliferative stages of healing farther out from an initial injury.
· Interpretations of the meaning of pain can drive behavior!6: For example, in a recent editorial, pain and fatigue have been examined as useful metrics to guide patient-clinician conversations. Specifically, patients’ beliefs about pain and fatigue may guide adaptive vs. maladaptive behaviors during rehabilitation. See graphic below:
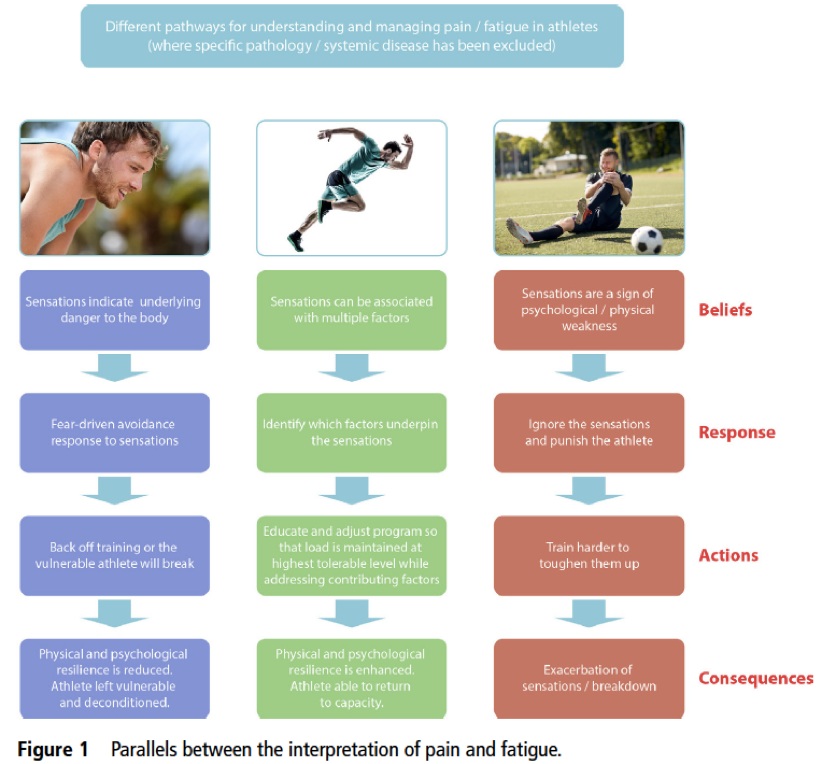
(Figure from O’Sullivan et al., 2018)6
Research tells us that there may also be utility in a more comprehensive discussion of pain such as that used in pain neuroscience education. Studies have shown pain neuroscience education to be a successful adjunct treatment to physical therapy in treating many different types of chronic pain conditions1,7.However, it is important to note that there may be limitations to its use as well. One recent study8 showed that two hours of pain education did not improve pain ratings in individuals with acute low back pain8. If you are interested in some expert clinical commentary on this study from physical therapist and renowned pain scientist, Dr. Lorimer Moseley, see: HERE and HERE.
The challenge that we face as clinicians is translating the science of pain and its technical language into digestible and useful information for patients. At the very least, we need to be aware of how we are communicating because the words and language we choose to use to educate our patients DO matter!9,10
Here are some foundational principles to keep in mind when discussing pain with your patients and how to translate those principles into patient friendly language 11,12,13,14.
THE “SCIENCE” FOR CLINICIANS:
Research Supported Tips for Pain Education11,12,13,14
- Keep it simple, use analogies and metaphors to teach about pain
- Make it relevant to the patient
- Pain does NOT equal pathology in all cases
- Patients CAN understand this stuff! (NPQ-12, Moseley reference)
- MANY factors influence pain
- Teaching about pain aligns with our mission as PTs to empower patients to improve their own health
THE “ART” OF TEACHING ABOUT PAIN:
Patient Friendly Sayings and Language:
There are many resources that can help in teaching about pain11,12,13,14 and here are a few of my favorite sayings/analogies to help patients understand how pain works:
“Hurt but not harm”
“Sore but safe”
“Pain is in the brain”* (Caveat here: without a good patient-clinician rapport this phrase can come off as pejorative and suggesting (although NOT the intent at all) that “it’s all in your head”, use this phrase with CAUTION and only with some patients)
“The issue may not be in the tissue”
“Pain is like an alarm system”
“Motion is lotion”
Good luck and please share below in the comments section any other sayings/strategies that you have found helpful in teaching about pain!
Check your Quiz Answers from above with the key below:
PAIN SCIENCE & CHRONIC PAIN RESOURCE HANDOUT FOR CLINICIANS (Updated February 2021):
PAIN SCIENCE & CHRONIC PAIN RESOURCE HANDOUT FOR PATIENTS (Updated February 2021):
References for this post:
1. Louw A, Puentedura EJ. Therapeutic Neuroscience Education: Teaching Patients About Pain. Minneapolis, Minnesota: Orthopedic Physical Therapy Products, 2013.
2. Catley MJ, O’Connell NE, Moseley GL. How Good Is the Neurophysiology of Pain Questionnaire? A Rasch Analysis of Psychometric Properties. The Journal of Pain. 2013;14(8):818-827.
3. Silbernagel KG, Thomeé R, Thomeé P, Karlsson J. Eccentric overload training for patients with chronic Achilles tendon pain—a randomized controlled study with reliability testing of the evaluation methods. Scand J Med Sci Sports. 2001;11:197-206.
4. Continuing Education Course: “Mastering Lower Limb Tendinopathy” by Dr. Peter Malliaras, PT, PhD: https://www.tendinopathyrehab.com/
5. Cyriax, JH. Textbook of Orthopaedic Medicine: Volume 1 Diagnosis of Soft Tissue Lesions Eighth Edition. London: Bailliere Tindall: 1982.
6. O’Sullivan K, O’Sullivan PB, Gabbett TJ. Pain and fatigue in sport: are they so different? British Journal of Sports Medicine. 2018;52(9):555-556.
7. Louw A, Zimney K, Puentedura EJ, Diener I. The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Physiotherapy Theory and Practice. 2016;32(5):332-355.
8. Traeger AC, Lee H, Hübscher M, et al. Effect of Intensive Patient Education vs Placebo Patient Education on Outcomes in Patients with Acute Low Back Pain: A Randomized Clinical Trial. JAMA Neurology. November 2018.
9. Bedell SE, Graboys TB, Bedell E, Lown B. Words That Harm, Words That Heal. Archives of Internal Medicine. 2004;164:4.
10. Stewart M, Loftus S. Sticks and Stones: The Impact of Language in Musculoskeletal Rehabilitation. Journal of Orthopaedic & Sports Physical Therapy. 2018;48(7):519-522.
11. Butler DS, & Moseley GL. Explain Pain: 2nd ed. Adelaide, Australia: NOI Group Publications; 2013.
12. Hanscom, D. Back In Control: A Surgeon’s Roadmap Out of Chronic Pain 2nd Ed. Seattle, Washington: Vertus Press; 2017.
13. Louw A. Why Do I Hurt? A Patient Book About The Neuroscience of Pain. Minneapolis, Minnesota: Orthopedic Physical Therapy Products; 2013.
14. Moseley, GL. Painful Yarns: Metaphors & Stories to Help Understand The Biology of Pain. Minneapolis, Minnesota: Orthopedic Physical Therapy Products; 2012.
